NCLEX preparation for international nurses begins with a fundamentally different starting point than it does for US-educated candidates — not because international nurses are less clinically skilled but because the examination they are preparing for measures clinical reasoning within a specific framework of US nursing practice standards, priority hierarchies, and clinical decision-making architecture that may differ meaningfully from the nursing education and practice context in which their clinical competency was built. A nurse who has practiced competently and safely in the Philippines, India, Nigeria, or the United Kingdom for years has genuine clinical expertise. What NCLEX preparation for that nurse requires is not building clinical expertise from scratch but systematically mapping existing clinical competency onto the specific reasoning frameworks, priority sequences, and communication principles that US nursing practice — and therefore the NCLEX — uses as its foundational structure.
The first-attempt pass rate for internationally educated nurses consistently runs 20 to 35 percentage points below the first-attempt pass rate for US-educated candidates — not because international nurses are less competent clinicians but because the preparation gap is specific and addressable: the NCLEX clinical reasoning framework is different from the clinical reasoning frameworks taught and practiced in most other healthcare systems, and NCLEX preparation that does not specifically address this framework gap will produce a well-prepared nurse who is underprepared for this specific examination regardless of how extensively they have studied the clinical content.
This guide addresses NCLEX preparation for international nurses from the beginning: the credential evaluation and eligibility process that precedes any preparation activity, the specific clinical reasoning gaps that international nurses most commonly encounter and that preparation must specifically address, the NGN clinical judgment framework that all nurses must understand for the current examination, the language and scenario interpretation challenges that English as a second or additional language introduces, the preparation resource selection principles for international candidates, and the realistic preparation timeline that the international nurse’s specific starting point requires. This is not a general NCLEX preparation guide repurposed for international candidates — it is a preparation framework built specifically around the international nurse’s distinct preparation needs.
Step 1: Credential Evaluation and Eligibility — Before Preparation Begins
NCLEX preparation for international nurses cannot begin productively until the credential evaluation and eligibility pathway is understood — because the timeline for credential evaluation directly determines the preparation timeline, and beginning intensive preparation before the eligibility process is underway produces a preparation period without a clear exam date endpoint.
The Credential Evaluation Process
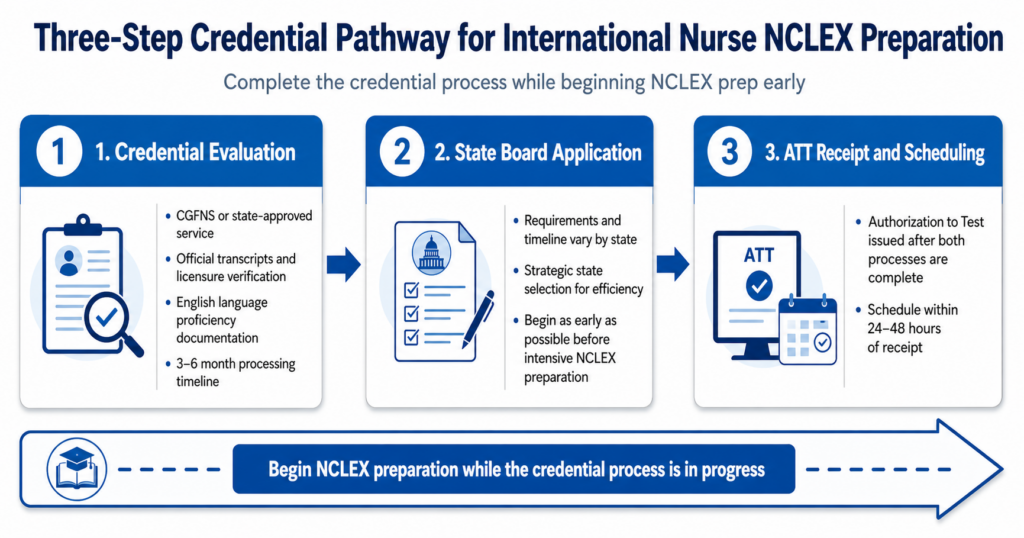
International nurses seeking NCLEX licensure in the United States must have their nursing education credentials evaluated by a recognized credential evaluation service to confirm that their nursing education is equivalent to US nursing program requirements. The most commonly used evaluation services for nursing credentials are the Commission on Graduates of Foreign Nursing Schools (CGFNS International) and its VisaScreen service for immigration-related licensure, and the state board of nursing in the target licensure state, which may require evaluation through CGFNS or may accept evaluations from other approved services depending on the state. The credential evaluation process involves submitting official transcripts from the nursing program, verification of licensure in the country of origin, and in many states a demonstration of English language proficiency through TOEFL or IELTS scores meeting the state’s minimum threshold. Processing timelines vary significantly by evaluation service and state board — CGFNS evaluations typically take three to six months for complete processing, and state board application reviews add additional time on top of the evaluation. Beginning the credential evaluation process as early as possible — ideally before beginning intensive NCLEX preparation — prevents the situation where a nurse has completed months of preparation but cannot schedule the exam because the credential process is still in progress.
State Board Selection and Application Strategy
Each US state’s board of nursing has its own requirements for international nurse licensure applications, and the variation between states is significant enough that state selection is a strategic decision for the international nurse beginning NCLEX preparation. States vary in their English language proficiency requirements (some require TOEFL or IELTS scores, others do not), their credential evaluation service requirements (some accept multiple services, others require CGFNS specifically), their processing timelines (some process applications within weeks, others take months), and their retake policies (the 45-day minimum between attempts is NCSBN-standard but additional state requirements vary). For international nurses whose primary goal is beginning US nursing practice as quickly as possible, selecting the state with the most efficient processing timeline for their specific credential background is a legitimate preparation strategy — licensure is portable through endorsement to other states once the initial license is obtained. Consult the NCSBN’s list of member boards at ncsbn.org and each state board’s website directly to compare current processing requirements and timelines for international applicants.
English Language Proficiency Assessment
For international nurses for whom English is not a first language, an honest self-assessment of English language proficiency as it relates specifically to NCLEX preparation is an essential early step. NCLEX preparation requires not only conversational English proficiency but clinical English proficiency — the ability to read and interpret complex clinical scenario descriptions under timed conditions, to distinguish subtle clinical language distinctions that determine the correct priority action, and to process the sophisticated medical and nursing terminology that the exam’s questions use without additional cognitive load from language processing. A nurse who reads English fluently in their first language but for whom English is an additional language should budget additional preparation time for clinical English vocabulary development and timed reading practice alongside the clinical content and reasoning preparation that all candidates require. The NCLEX preparation timeline for international nurses whose clinical English proficiency requires development is typically longer than the standard six-to-eight week intensive — twelve to sixteen weeks is more realistic when clinical English proficiency development is incorporated into the preparation architecture.
Step 2: Understanding the Clinical Reasoning Framework Gap
The most important preparation insight for international nurses beginning NCLEX preparation is that the exam does not primarily test clinical knowledge — it tests clinical reasoning within a specific US nursing framework. Understanding what that framework is, how it differs from the clinical reasoning framework used in the nurse’s home country practice, and how to map their existing clinical competency onto the US framework is the preparation work that most distinguishes successful international NCLEX preparation from preparation that accumulates clinical content without building the reasoning framework the exam actually measures.
The Priority Hierarchy Difference
The NCLEX clinical reasoning framework organizes nursing priorities in a specific three-tier hierarchy — ABCs (airway, breathing, circulation) at the highest tier, Maslow’s physiological and safety needs at the second tier, and psychosocial needs at the third tier — and expects every nursing priority decision to be made by applying this hierarchy in sequence. This priority structure is explicitly taught in US nursing education and is the organizing framework for the most common question type on the NCLEX. Many international nurses arrive at NCLEX preparation having practiced in healthcare systems that organize clinical priorities differently — systems where patient family needs, hierarchical physician authority, or community-based care models influence priority decisions in ways that the NCLEX’s individual patient-centered physiological priority hierarchy does not accommodate. A nurse whose clinical instinct is to involve the family or defer to the physician order before completing the physiological assessment that the NCLEX expects first will consistently miss priority questions not from lack of clinical knowledge but from applying a different priority hierarchy than the exam uses. NCLEX preparation for international nurses must explicitly map their existing priority reasoning onto the US three-tier hierarchy and practice applying it across clinical scenarios until it becomes the automatic framework rather than the consciously retrieved rule.
The Nursing Process Autonomy Assumption
A second clinical reasoning framework difference that international nurses frequently encounter in NCLEX preparation is the examination’s assumption of nursing autonomy in clinical decision-making — the expectation that the nurse independently assesses, identifies priorities, and initiates appropriate evidence-based interventions within their nursing scope of practice without awaiting physician direction. In many international healthcare systems, nursing practice is more hierarchically structured — nurses are expected to implement physician orders rather than independently initiating nursing actions. The NCLEX scenario that asks what the nurse does first when a patient presents with a specific clinical finding expects the candidate to select an independent nursing assessment or intervention rather than contact the physician as the first step, even when physician notification will eventually be appropriate. International nurses whose clinical practice has been primarily physician-order-driven will find that calling the physician is rarely the correct first nursing action on the NCLEX regardless of the clinical severity of the finding — because the exam’s first-action question is almost always answered by the assessment or intervention that the nurse independently performs before notification. Recognizing this autonomy assumption explicitly and practicing it across clinical scenarios is a specific NCLEX preparation requirement for international nurses that US-educated candidates rarely need.
Therapeutic Communication as a Clinical Skill
Therapeutic communication questions represent a substantial proportion of NCLEX preparation content that international nurses often underestimate — in part because communication skills feel less testable than clinical knowledge and in part because the specific communication techniques that the NCLEX defines as therapeutic reflect a patient-centered, empowerment-focused communication philosophy that is culturally specific to US nursing practice. International nurses from healthcare cultures with more paternalistic, directive, or family-mediated communication norms may find that their instinctive communication responses — which are professionally appropriate in their home practice context — are consistently marked as non-therapeutic on the NCLEX because they involve directing the patient’s decision, involving the family as the primary communication partner, or providing advice rather than facilitating the patient’s own expression. NCLEX preparation for international nurses must include explicit study of the therapeutic communication techniques defined by the NCSBN — open-ended questioning, reflection, clarification, focusing, silence — and specific practice identifying non-therapeutic responses (false reassurance, advice-giving, changing the subject, minimizing) as the distractors they are in a US nursing context regardless of how appropriate those responses might be in other clinical communication cultures.
Step 3: The NGN Clinical Judgment Framework for International Nurses

The Next Generation NCLEX format launched in 2023 added a layer of NCLEX preparation complexity that affects all candidates — but affects international nurses specifically because the CJMM clinical judgment framework the NGN formats test reflects US nursing education’s specific approach to clinical decision-making documentation and explicit reasoning articulation.
Understanding the CJMM for the International Nurse
The Clinical Judgment Measurement Model organizes clinical decision-making into six sequential cognitive skills: recognize cues (identifying relevant clinical data from the scenario), analyze cues (interpreting what the identified data means clinically), prioritize hypotheses (ranking possible explanations by urgency), generate solutions (identifying potential nursing actions), take action (selecting the most appropriate action for the current clinical moment), and evaluate outcomes (assessing whether the nursing action achieved the intended result). This six-step articulation of clinical reasoning is a formal model that US nursing education explicitly teaches, and NCLEX preparation resources built for US candidates assume familiarity with this model as a frame of reference for understanding NGN question formats. International nurses beginning NCLEX preparation may have well-developed clinical judgment that intuitively operates through similar steps but have never encountered this explicit six-step articulation — which means the NGN format’s question design will be opaque without the CJMM framework as a guide. Beginning NCLEX preparation with deliberate study of the CJMM — using the NCSBN’s official CJMM documentation at ncsbn.org — before beginning NGN format practice questions is strongly recommended for international nurses who have not previously encountered this framework.
NGN Format Practice Priorities for International Nurses
The five NGN format types — extended multiple response, matrix multiple response, bow tie, drop-down cloze, and trend questions — each require format-specific orientation that international nurses need to address explicitly in NCLEX preparation. The unfolding case study set is the NGN format most likely to challenge international nurses for two distinct reasons. First, the scenario progressively reveals clinical data across multiple questions, requiring the candidate to carry forward an accumulating clinical picture rather than reading each question as a standalone scenario — which requires a sustained narrative clinical reasoning approach that differs from the question-by-question pattern matching that traditional multiple choice preparation builds. Second, the clinical decisions tested within unfolding case study sets assume US nursing autonomy and priority hierarchy norms — a nurse who defaults to physician notification as the priority action across case study take-action questions will consistently score below standard regardless of correct case-set integration. The NCSBN official NGN sample questions at ncsbn.org provide the most authoritative format orientation for international nurses beginning NGN-specific NCLEX preparation — completing these samples early in the preparation period establishes realistic expectations about the format complexity and the clinical reasoning depth the current examination requires.
Partial Credit Mechanics and Response Strategy
The NGN partial credit scoring mechanics — where selecting all correct options without selecting any incorrect options produces full credit, selecting some correct options produces partial credit, and selecting incorrect options reduces the score — require a specific response strategy that international nurses must understand before beginning NGN format practice. The optimal response strategy is applying the clinical reasoning criteria for each option independently rather than comparatively — evaluating whether each option meets the clinical criteria for correctness given the scenario data before considering whether it should be included relative to other options. International nurses accustomed to single-best-answer traditional multiple choice formats may instinctively apply comparative reasoning (this option is better than that option) rather than independent criteria reasoning (this option meets the clinical criteria for inclusion; this other option also meets the criteria independently). The NCLEX preparation practice that builds independent criteria reasoning — applied to every option in every extended multiple response or matrix question — produces the partial credit optimization that the format rewards.
Step 4: Building the International Nurse NCLEX Preparation Plan
The NCLEX preparation plan for international nurses is structurally different from the standard preparation timeline in three specific ways: it is typically longer (to accommodate framework gap addressing and clinical English development), it allocates preparation time differently (prioritizing framework and format orientation before content coverage), and it includes preparation activities specific to the international nurse context that standard preparation guidance does not address.
The Realistic Timeline for International NCLEX Preparation
International nurses whose primary preparation challenges are clinical reasoning framework gaps and NGN format orientation — rather than clinical English language development — should plan a twelve-week minimum NCLEX preparation timeline from beginning to exam date. The first two weeks are orientation weeks — studying the NCLEX clinical reasoning framework (three-tier priority hierarchy, nursing process autonomy assumption, therapeutic communication technique framework), completing the NCSBN official NGN samples for format orientation, and completing a comprehensive diagnostic assessment that establishes the baseline performance profile. Weeks three through eight are the intensive preparation phase — targeted framework application practice using the gap types identified in the diagnostic assessment as the allocation guide, with 30 to 35 percent NGN format content in every session and deliberate framework application habit development. Weeks nine through eleven are the consolidation and simulation phase — weekly full simulations with framework application confirmation, accuracy trend verification against the four readiness benchmarks, and targeted intervention for any persistent below-standard categories. Week twelve is the final calibration week — the standard last-week protocol with taper, final simulation, logistics confirmation, and exam morning preparation. For international nurses whose clinical English development is a significant component of NCLEX preparation, extending the timeline to sixteen weeks with two to four weeks of clinical English vocabulary and timed reading practice incorporated before the intensive preparation phase begins is more realistic than attempting the twelve-week timeline with language development included.
Content Priority Allocation for International Nurses
The content priority allocation for international NCLEX preparation differs from the standard allocation in that framework-gap content areas receive higher relative priority than their test plan weighting alone would suggest. Medical-surgical nursing — the largest test plan content area — should receive standard high-priority allocation for international nurses as for all candidates. However, the priority framework application practice that international nurses need is not content-specific — it must be deliberately applied across all content area sessions from week one to build the automatic framework reasoning that the exam requires. Mental health nursing receives higher relative priority for international nurses than for US-educated candidates because therapeutic communication questions represent a disproportionate challenge for nurses from non-US communication cultures and because mental health scenarios frequently involve the most culturally specific applications of the therapeutic communication framework. Community health and health promotion content — which the April 2026 test plan updated to include expanded social determinants of health scope — receives moderately higher priority for international nurses from healthcare systems where community-based care models differ significantly from US public health nursing practice.
The Framework Mapping Practice
A specific NCLEX preparation activity for international nurses that has no equivalent in standard preparation guidance is the framework mapping practice — a deliberate exercise conducted at the beginning of the preparation period that explicitly maps the nurse’s existing clinical reasoning patterns onto the US nursing framework before practicing any questions. The exercise proceeds in three steps. Step one: for five to ten clinical scenarios the nurse would encounter in their home practice, write out the priority nursing action they would take using their existing clinical framework — the actual response that professional experience and training would produce in their healthcare context. Step two: apply the US three-tier priority hierarchy to the same scenarios and identify what the NCLEX-aligned priority nursing action would be — and where it differs from the home-practice response. Step three: for each scenario where a difference exists, identify the specific framework principle that produces the US-aligned response and name it (ABC-tier threat present: airway first regardless of other findings; psychosocial need present alongside unaddressed physiological need: physiological first regardless of how compelling the communication opportunity appears). This framework mapping exercise makes the reasoning framework difference explicit and actionable before the diagnostic assessment establishes the performance baseline — which means the first weeks of NCLEX preparation are directed at closing the gap that the framework analysis reveals rather than accumulating question volume that the framework gap will continue to produce wrong answers across.
Step 5: Language and Scenario Interpretation for International Nurses
Clinical English proficiency in NCLEX preparation is more specific than general English fluency — it requires the ability to interpret clinical scenario language under timed conditions with sufficient precision to identify the clinically critical data that determines the correct reasoning path.
High-Stakes Clinical Language Distinctions
The NCLEX clinical scenario language uses specific vocabulary distinctions that carry different clinical implications and must be interpreted precisely rather than approximately. The distinction between acute and chronic, between new onset and baseline, between expected and unexpected, and between worsening and stable are the clinical language discriminations that most frequently determine whether a scenario presents a clinical emergency requiring immediate priority action or a managed condition requiring monitoring and routine assessment. International nurses whose English clinical reading is at a general comprehension level but not at the precise discrimination level may process a scenario correctly at the narrative level — understanding what is happening to the patient — without correctly identifying the specific clinical language distinction that makes one option the priority over three equally reasonable-appearing alternatives. NCLEX preparation for international nurses should include deliberate clinical language precision practice — reading scenarios and explicitly naming the specific clinical language discriminations present (this is acute, not chronic — that changes the priority; this finding is new, not baseline — that changes the framework) before engaging any answer options.
Medical Terminology Variants Across Healthcare Systems
International nurses may encounter NCLEX preparation scenarios that use US medical terminology for conditions, medications, or procedures that are named differently in their home country’s clinical practice. The beta-blocker metoprolol that appears commonly in NCLEX pharmacology scenarios is the same medication as the Lopressor that US brand-name practice references — but an international nurse whose pharmacology education used a different generic name or a different brand-name convention may not recognize the medication in a clinical scenario that names it differently. Similarly, clinical condition terminology varies across healthcare systems: what is called acute coronary syndrome in US clinical nomenclature may be referred to differently in other systems, and the subtle presentation difference between STEMI and NSTEMI that NCLEX preparation pharmacology requires knowing may be taught with different emphasis or terminology in non-US nursing education. Identifying and addressing these terminology variant gaps early in NCLEX preparation prevents the frustration of incorrect answers produced by terminology unfamiliarity rather than clinical reasoning failures during the intensive preparation phase.
Timed Reading Practice Under Exam Conditions
For international nurses for whom English is an additional language, adding deliberate timed reading practice to NCLEX preparation produces the exam-condition language processing speed that timed practice questions alone cannot develop. The 90-second per question average that the NCLEX requires allocates approximately 30 to 40 seconds for stem reading and clinical data extraction, 30 to 40 seconds for option evaluation, and 10 to 20 seconds for final selection and submission. A nurse who requires 60 seconds to read and process the stem is beginning option evaluation with only 30 seconds remaining — which produces either rushed reasoning or time budget violations that accumulate across the session into clock pressure. Timed reading practice — reading clinical scenario stems and extracting the clinically critical data within 30 to 35 seconds as a deliberate daily practice — builds the language processing speed that exam-condition NCLEX performance requires. This practice is distinct from question bank practice and should be added specifically for international nurses who identify timed reading speed as a NCLEX preparation challenge during the diagnostic assessment phase.
- Resource selection for international NCLEX preparation: Prioritize question banks with both traditional and NGN format items updated for the current test plan — UWorld, Kaplan, and ATI are the most commonly used by international nurses with established track records. The NCSBN’s own Learning Extension offers content specifically aligned with the NCSBN test plan. For clinical English development, medical terminology courses designed for healthcare professionals rather than general English language courses produce the clinical vocabulary precision that NCLEX preparation requires. For framework orientation, NCLEX-specific review books organized around the clinical reasoning frameworks (priority hierarchy, nursing process, therapeutic communication) rather than by body system provide the framework architecture that content-organized resources do not.
- Community and peer support for international nurses: International nurse NCLEX preparation communities — available through professional organizations including the Philippine Nurses Association of America, the Organization of Nigerian Nurses and Midwives, and international nursing forums — provide peer preparation support, shared resource recommendations, and the social accountability that sustains preparation quality across a long preparation timeline. International nurses whose primary peer group has already passed the NCLEX or is not preparing simultaneously benefit especially from connecting with peers at a similar preparation stage, even in online or virtual community contexts.
When to seek targeted tutoring as an international NCLEX candidate: International nurses who identify a persistent clinical reasoning framework gap — consistently selecting physician-notification options as the first nursing action, consistently selecting psychosocial options before physiological needs are addressed, or consistently missing therapeutic communication questions despite content knowledge — benefit most from diagnostic tutoring that can observe their reasoning process in live verbalization sessions. Self-directed preparation can identify that a framework gap exists through error type classification; it typically cannot identify the specific clinical context or reasoning trigger that produces the framework application failure without external observation.
Conclusion
NCLEX preparation for international nurses is a specific preparation challenge that general NCLEX guidance does not fully address — and the pass rate data consistently confirms the cost of treating it as equivalent to US-educated candidate preparation. The clinical reasoning framework gaps (priority hierarchy, nursing process autonomy, therapeutic communication), the NGN clinical judgment format challenges (CJMM orientation, unfolding case study integration, partial credit mechanics), the language precision requirements, and the credential eligibility process all require specific, deliberate preparation investments that the standard NCLEX preparation framework does not include. None of these challenges are beyond addressing. All are specific, identifiable, and closable through the preparation approach this guide describes.
The international nurse who begins NCLEX preparation with a clear understanding of the framework gap between their home-practice clinical reasoning and the US nursing framework, a realistic preparation timeline that accommodates the specific preparation work required, and a deliberate orientation to the NGN clinical judgment framework before beginning clinical content practice is not at a preparation disadvantage relative to the US-educated candidate. They are building on a foundation of genuine clinical expertise — applying it to the specific reasoning framework that the NCLEX measures. That is not a handicap. With the right preparation structure, it is a significant strength.