How to Pass the NCLEX as a Repeat Test Taker (2026 Ultimate Guide)
Updated: 2026 | Estimated Reading Time: 11 minutes
The repeat NCLEX test taker occupies a uniquely challenging position in the preparation landscape — not because a second or third attempt is unusual (roughly 15 to 20 percent of US-educated candidates do not pass on their first attempt) but because the repeat test taker is preparing for the same examination with the specific psychological burden of a previous failed result, a preparation approach that did not produce a passing outcome, and the urgent need to identify what was different about that preparation rather than simply repeating it with more intensity. The NCLEX test taker who returns for a second attempt with the same study plan, the same resources, and the same preparation behaviors that preceded the first attempt is not preparing for the next exam — they are rehearsing the same outcome. Different results require different approaches, and the most important work a repeat NCLEX test taker can do before beginning any study activity is understanding precisely what the first attempt revealed about the gaps that the preparation did not close.
This guide is written specifically for the repeat NCLEX test taker — not the candidate who has read general preparation guidance and is wondering if it applies to them but the candidate who has sat the exam, received a not-passing result, and is now standing at the beginning of a second preparation period knowing that something needs to change but uncertain what that something is. The guidance here addresses the specific challenges that distinguish repeat test taker preparation from first-attempt preparation: the CPR analysis that transforms a failure result into the most specific preparation intelligence available, the structural change imperative that makes the second attempt different from the first rather than more intense, the psychological management of the performance anxiety that previous failure generates, and the specific preparation behaviors that most reliably produce passing results for the repeat NCLEX test taker who implements them with full commitment and quality discipline. This guide is organized as a complete framework — from the first days after a not-passing result through the day before the second attempt — covering every preparation phase, every decision point, and every specific technique that distinguishes the repeat NCLEX test taker preparation approaches that produce passing results from those that reproduce the same outcome as the first attempt.
Understanding Why Repeat Test Taker Preparation Fails Most Often
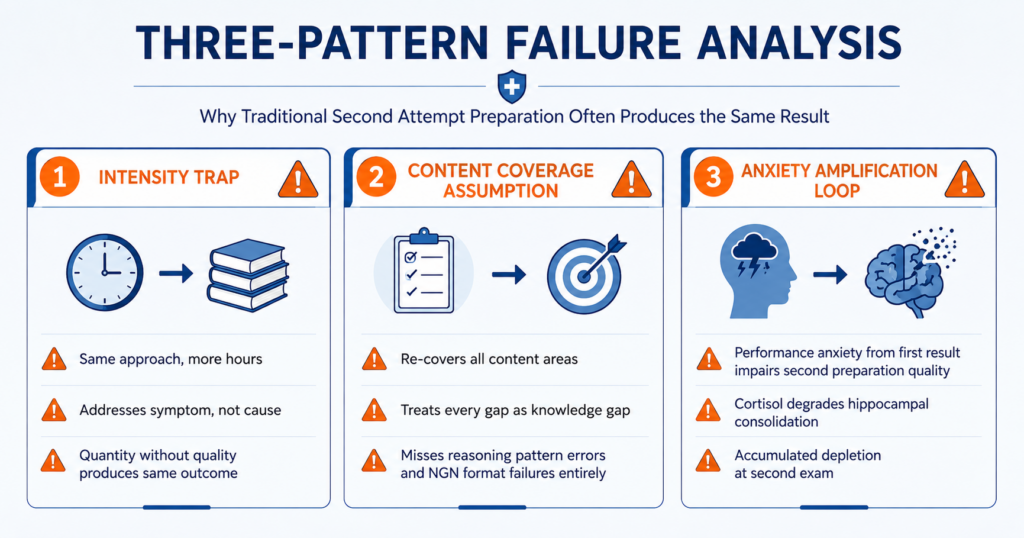
Before building the second-attempt preparation strategy, every repeat NCLEX test taker needs to understand the specific failure patterns that most commonly produce a second not-passing result — because identifying which pattern applies to their situation determines what the second preparation must do differently.
Failure Pattern 1: The Intensity Trap
The most common repeat NCLEX test taker preparation failure is the intensity trap — the response to a first not-passing result that consists of exactly the same preparation approach applied with more hours, more questions, more content review, and more determination. This response is emotionally understandable: the candidate who did not pass the first time experienced the exam as harder than their preparation predicted, and the logical conclusion is that more preparation would have been sufficient. The problem is that preparation quantity did not predict the first outcome and will not reliably predict the second. If the first attempt produced below-standard performance in specific content categories, studying those same categories with the same approach for more hours addresses the symptom (insufficient performance) without addressing the cause (incorrect preparation approach, reasoning pattern error, or wrong intervention type for the identified gap). The repeat NCLEX test taker who recognizes they are in the intensity trap asks a different question than how much more do I need to study — they ask what specifically did my approach fail to develop and what different approach would address that specific failure.
Failure Pattern 2: The Content Coverage Assumption
The second common repeat NCLEX test taker failure pattern is the content coverage assumption — the belief that the first attempt produced a not-passing result because certain clinical content areas were not sufficiently covered and that comprehensive re-coverage of all content areas is the correct second-attempt response. This assumption fails for the same reason it fails in first-attempt preparation: the NCLEX does not test content recognition, it tests clinical reasoning application. A repeat NCLEX test taker who reviews cardiovascular pharmacology for the second time and can now list digoxin toxicity signs more completely than before has improved content recognition without necessarily improving the clinical reasoning that applies that content correctly in a novel patient scenario. The CPR data tells the repeat test taker which content areas fell below the passing standard. It does not tell them why — whether the gap is a knowledge gap requiring content review, a reasoning pattern error requiring behavioral correction, or a NGN format application failure requiring format-specific practice. The content coverage assumption answers only the knowledge gap question and misses the other two entirely.
Failure Pattern 3: The Anxiety Amplification Loop
A third repeat NCLEX test taker failure pattern is the anxiety amplification loop — where the performance anxiety generated by the first not-passing result impairs the second preparation’s quality and the second exam’s performance, producing a second not-passing result that increases the anxiety further, which impairs the third preparation even more severely. This loop is clinically real: cortisol elevation from sustained performance anxiety directly impairs hippocampal memory consolidation, reducing the clinical reasoning development that preparation sessions produce regardless of how many hours are invested. The repeat NCLEX test taker who completes every preparation session in a state of anxious urgency, whose sleep is disrupted by rumination about the second result, and who arrives at the second exam with weeks of accumulated cognitive depletion is not better prepared than the candidate who completed fewer hours of preparation with adequate recovery and psychological management. The anxiety amplification loop is a preparation variable, not a personality trait — and it responds to the specific physiological and cognitive management practices described in this guide.
Phase 1: The CPR Analysis (Days 1 Through 7 After the Result)

The Candidate Performance Report is the most valuable document a repeat NCLEX test taker receives — not despite being the record of a failed examination but because of it. No diagnostic practice assessment, no question bank analytics report, and no practice simulation provides clinical performance data with the specificity, accuracy, and relevance of actual NCLEX performance data. The CPR tells the repeat test taker what their actual clinical reasoning produced at actual exam difficulty under actual exam conditions — which is precisely the information that second-attempt preparation needs as its foundation.
Reading the CPR as a Preparation Prescription
The CPR categorizes performance in each content category as near passing standard, above passing standard, or below passing standard. The repeat NCLEX test taker reading the CPR as a preparation prescription extracts three specific analyses from this data. First, the scope analysis: how many categories are below passing standard versus at or above? A CPR with two below-standard categories and seven above-standard requires a far more targeted second preparation than a CPR with six below-standard categories. The scope analysis defines the preparation budget before any content allocation decisions are made. Second, the pattern analysis: do the below-standard categories cluster in a way that suggests a common cause? Below-standard performance across cardiovascular, respiratory, and critical care simultaneously may indicate a physiological priority framework error appearing across all high-acuity scenarios rather than three separate content knowledge gaps. Below-standard performance in pharmacology and mental health simultaneously may indicate a reasoning pattern affecting medication safety and communication scenarios across content areas. Pattern identification in the CPR data often reveals that what appears to be multiple content gaps is actually a single cross-cutting reasoning error. Third, the consistency analysis for repeat test takers with multiple CPRs: which categories were below standard on both the first and second CPR? Categories that are below standard across multiple attempts despite preparation targeting them in between are the highest-priority investigation targets — they are maintained by something the previous preparation has not addressed.
The Gap Type Classification for Each Below-Standard Category
For every content category identified as below passing standard in the CPR, the repeat NCLEX test taker must classify the gap type before selecting the preparation intervention. The three gap types — knowledge gap, reasoning pattern error, and approach methodology failure — each require a different intervention, and applying the wrong intervention to any gap type produces preparation activity without preparation improvement. Knowledge gap diagnosis: was the clinical content in this category genuinely absent from the accessible knowledge base during the exam, or was it present but misapplied? Review five to ten practice questions in this category from the period before the first attempt and examine the rationales — if the rationales consistently teach clinical principles that were genuinely unknown, the gap is a knowledge gap requiring content review before returning to practice. Reasoning pattern error diagnosis: if the rationales reveal clinical principles that were known but not applied correctly — the content was recognizable in the rationale but the scenario presentation produced an incorrect reasoning path — the gap is a reasoning pattern error requiring specific behavioral correction practice rather than additional content review. Approach methodology failure diagnosis: if performance in this category during preparation was adequate (above 50 percent) but the CPR shows below-standard performance on the actual exam, the gap is an approach methodology failure — likely the cognitive stamina, pacing, or anxiety management dimension that impaired performance under actual exam conditions despite adequate preparation performance.
Building the Second-Attempt Timeline
The CPR analysis produces the second-attempt preparation timeline by mapping the identified gaps to the intervention types they require and the estimated time each intervention needs to produce measurable improvement. Knowledge gaps in one to two content categories require one to two weeks of targeted content review followed by two to three weeks of practice question sessions testing application of that content. Reasoning pattern errors require one to two weeks of deliberate behavioral correction practice to begin automating the correction and two to three weeks of mixed-content sessions confirming transfer. Approach methodology failures require sustained physiological and psychological management across the full preparation period with specific exam-day protocol preparation in the final week. The repeat NCLEX test taker builds their second-attempt timeline by stacking these interventions into the available preparation weeks — prioritizing the interventions for CPR-identified below-standard categories that appeared on both the first and second CPR, then second-priority interventions for categories below standard only on the most recent CPR.
Phase 2: Building the Structurally Different Second Preparation (Weeks 1 Through 4)
The preparation prescription derived from the CPR analysis must be structurally different from the first attempt’s preparation in ways that specifically address the identified gap types — not marginally different in volume or resource selection but fundamentally different in methodology and approach.
The Structural Change Audit
Before any second-attempt preparation activity begins, the repeat NCLEX test taker conducts a structural change audit — a systematic comparison of what the first preparation did and what the second preparation will do differently for each identified gap. For each below-standard CPR category, the audit asks and answers: what did the first preparation do in this area, what gap type was present in this area, and what different approach does that gap type require? A knowledge gap category that received insufficient content review in the first preparation needs specific content review sessions before practice question sessions in the second. A reasoning pattern error category that received the same generic practice sessions as all other categories in the first preparation needs deliberate behavioral correction practice with the specific error type correction applied to every question in the second. An approach methodology failure category that performed adequately in preparation but not on the exam needs exam-simulation-condition practice with the specific physiological and anxiety management protocol built in. The structural change audit produces a concrete, specific description of how the second preparation differs from the first for each gap identified — which is the most direct protection against the intensity trap and content coverage assumption failure patterns.
The Deliberate Correction Practice Protocol
For reasoning pattern errors identified through the CPR analysis and gap type classification, the repeat NCLEX test taker applies the deliberate correction practice protocol — a targeted behavioral habit-building practice that is distinct from standard question bank sessions. The protocol selects 25 to 30 questions per session in the identified content area and applies the specific behavioral correction to every question before engaging any answer option — not just to questions that feel relevant to the identified error type but to every question in the session. This universal application accelerates the automation of the correction habit faster than selective application because the behavioral habit fires every time regardless of whether the specific error type is triggered by any given question. The session is followed by the self-monitoring protocol: for each question, did the correction fire before reading options, during option evaluation, or not at all? The self-monitoring data — recorded and reviewed weekly — confirms whether the correction habit is automating and identifies the specific clinical contexts where it is still failing to transfer. This precision is what the second NCLEX test taker preparation produces that generic additional question practice cannot.
The NGN-Specific Second Preparation for Repeat Test Takers
Every repeat NCLEX test taker should include NGN-specific gap analysis as a component of their second preparation regardless of whether the CPR explicitly identifies NGN format performance as a concern. The CPR does not separately report NGN format accuracy from traditional format accuracy — it reports content category performance that combines both format types. A repeat NCLEX test taker whose content category performance fell below standard may have a knowledge gap, a reasoning pattern error, or a NGN format application failure whose contribution to the below-standard performance is invisible in aggregate category data. Tracking NGN accuracy separately throughout the second preparation — maintaining a separate weekly NGN accuracy count alongside the overall accuracy trend — provides the visibility into NGN performance that the CPR cannot. Completing the NCSBN official NGN sample questions at ncsbn.org at the start of the second preparation establishes the most accurate NGN format baseline available and identifies whether format-specific preparation is a priority need before the second attempt.
Phase 3: Managing Performance Anxiety as a Preparation Variable (Throughout)
Performance anxiety in the repeat NCLEX test taker is not the same as first-attempt pre-exam anxiety. It carries the weight of a confirmed disappointing result, the social dimension of peers who have moved on to nursing practice, and the fear that a second failure will raise questions about nursing fitness that a first failure did not. Managing this specific form of anxiety is not a wellness activity supplementary to preparation — it is a core preparation requirement whose neglect directly impairs the clinical reasoning development that the second preparation is designed to produce.
The Failure Reframe: What the First Attempt Actually Proved
The most important cognitive reframe for the repeat NCLEX test taker managing performance anxiety is a precise, accurate assessment of what the first attempt actually proved — as opposed to what the emotional experience of the result felt like it proved. A not-passing result proves that the clinical reasoning competency demonstrated through the response pattern on the first attempt did not place the ability estimate above the passing standard on that occasion. It does not prove: that the candidate is not intelligent enough to be a nurse, that the candidate does not have the clinical knowledge to practice safely, that nursing is the wrong career for this person, or that a second attempt will produce the same result. It proves a specific, measurable gap between the first preparation’s clinical reasoning development and the passing standard — a gap that is identifiable from the CPR data, targetable through structured second preparation, and closable within six to eight weeks of deliberate corrective work. The repeat NCLEX test taker who carries this precise assessment of what the first attempt proved into the second preparation is far better equipped to manage the performance anxiety it generates than one who carries the global failure narrative.
The Physiological Management Protocol for Repeat Test Takers
The physiological management protocol for the repeat NCLEX test taker is identical in structure to the burnout prevention protocol described elsewhere in this series but applies with greater urgency given the anxiety amplification loop risk specific to repeat preparation. Two non-preparation days per week are non-negotiable — not reduced-intensity days but complete rest from all NCLEX preparation activity. Thirty minutes of aerobic physical activity on five of seven preparation days reduces cortisol, activates BDNF that supports the hippocampal memory consolidation the second preparation requires, and produces the dopaminergic activation that counteracts the motivational depletion that anxiety generates over weeks. Seven to eight hours of sleep every night — not as an aspiration but as the non-negotiable physiological foundation of clinical reasoning development — must be protected against the ruminative anxiety that keeps repeat test takers awake rehearsing exam scenarios and preparation regrets. Each of these physiological investments is preparation infrastructure for the repeat NCLEX test taker in a more literal sense than for first-attempt candidates: the anxiety amplification loop that destroys second preparations operates through the physiological mechanisms that these interventions directly address.
The Progress Documentation Practice
The progress documentation practice is a specific repeat NCLEX test taker anxiety management tool that replaces the vague subjective sense of whether preparation is going well with concrete, verifiable weekly evidence of clinical reasoning improvement. Every Sunday, record five specific data points: total questions completed, overall accuracy trend compared to the previous week, content category accuracy for each CPR-identified below-standard area, NGN accuracy tracked separately, and the self-monitoring data from the deliberate correction practice sessions. This documentation converts the anxiety’s recurring question of am I doing enough into the answerable analytical question of what does the data show about this week’s preparation progress. When the data shows upward trends in the below-standard categories and self-monitoring data showing the correction habit automating, the answer to whether preparation is working is visible rather than felt. The visible answer reliably produces less anxiety than the invisible one — which is why the progress documentation practice is anxiety management as much as it is preparation management.
Conclusion
The repeat NCLEX test taker who passes their second or third attempt does not pass because they studied harder than they did the first time. They pass because they understood what the first attempt revealed through CPR analysis, because they built a second preparation that addressed the specific gap types that analysis identified rather than repeating the first approach with more intensity, because they managed the performance anxiety that a previous failed result generates as a preparation variable rather than suppressing it or surrendering to it, and because they made the proceed decision based on benchmark data that confirmed their CPR-identified gaps had been specifically closed rather than on timeline pressure or financial urgency.
The first attempt was not wasted preparation. It was the most specific clinical reasoning gap data any nursing candidate can obtain — a performance record from the actual examination under actual conditions identifying exactly what needs to be different. The repeat NCLEX test taker who reads that data accurately, responds to it structurally rather than intensively, and arrives at the second attempt with genuine clinical reasoning improvement in every CPR-identified category is the NCLEX test taker most likely to pass. That is the path this guide has described. It is available to every candidate willing to walk it.