Nursing school does a great deal right. It builds the clinical knowledge base that NCLEX preparation depends on, develops the professional identity that nursing practice requires, and produces graduates whose commitment to patient care is evident in every clinical rotation. What nursing school does not always do — through no fault of faculty or curriculum design — is explicitly teach the specific clinical reasoning framework that the NCLEX examination uses to organize and test that clinical knowledge. The gap between nursing school preparation and NCLEX preparation is not a gap in clinical content. It is a gap in the specific reasoning architecture the examination measures — and filling it is what NCLEX preparation is actually for.
This matters because nursing students who assume their nursing school academic success will transfer directly to NCLEX performance are frequently surprised to discover that the study habits and reasoning approaches that produced excellent grades are not the same ones that produce strong NCLEX practice question accuracy. Students who graduated with GPAs in the top quartile of their class and found themselves struggling in early NCLEX preparation are not discovering that they are less clinically competent than their grades suggested. They are discovering that nursing school and the NCLEX are measuring overlapping but meaningfully different competencies — and that the gap between them is specific, addressable, and important to understand before preparation begins.
This guide identifies the eight most important things nursing school does not always teach about the NCLEX and its preparation — not as a criticism of nursing education but as a practical preparation supplement that fills the specific gaps between what nursing school provides and what NCLEX preparation requires. Understanding these gaps before beginning preparation allows candidates to allocate preparation time more efficiently toward what the examination actually measures rather than toward reinforcing what nursing school already developed.
Gap 1: The Explicit Three-Tier Priority Framework
What Nursing School Teaches
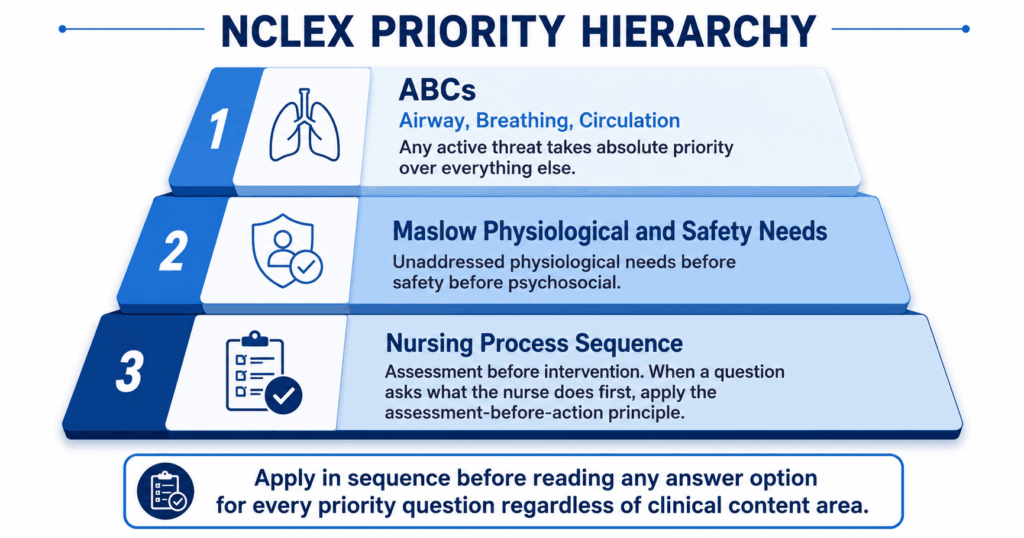
Nursing school teaches clinical priorities in the context of specific content areas — cardiovascular patients need oxygen and hemodynamic monitoring, neurological patients need frequent neuro checks, postoperative patients need pain management and early ambulation. These priorities are taught within the clinical context that produces them, and students develop strong implicit clinical judgment about which patients need attention in the clinical settings their rotations cover. What nursing school rarely teaches explicitly is the universal three-tier priority hierarchy that the NCLEX applies to every priority question across every clinical content area: ABCs first (any active threat to airway, breathing, or circulation takes absolute priority), Maslow’s physiological and safety needs second (unaddressed physiological needs take priority over psychosocial needs), and the nursing process sequence third (assessment before intervention when the question asks what the nurse does first). This framework is so fundamental to NCLEX preparation that every priority question — regardless of clinical content — is answered by applying it in sequence before engaging any answer option.
Why This Gap Matters for NCLEX Preparation
Nursing students who have not learned this explicit three-tier hierarchy consistently miss priority questions not because they lack clinical knowledge but because they apply clinical knowledge without a universal priority organizing framework — which produces correct answers for familiar clinical scenarios and incorrect answers when the same framework is required in an unfamiliar clinical combination. A nursing student who knows that a patient with COPD needs careful oxygen titration, that a patient in acute respiratory distress needs immediate intervention, and that a patient with family concerns needs therapeutic communication has the content knowledge for all three scenarios. Without the explicit three-tier framework, they may select the therapeutic communication option when the respiratory distress is the ABC-tier priority. With the framework applied automatically before options are read, the respiratory distress is identified as the ABC-tier threat that takes absolute priority over both the COPD management question and the family communication need. NCLEX preparation must specifically teach and practice this framework as a clinical reasoning tool rather than assuming nursing school’s implicit priority teaching has made it automatic.
Gap 2: The NCLEX Accuracy Standard vs. Nursing School Passing Standards
What Nursing School Teaches
Nursing school examinations have a defined passing threshold — typically 75 to 80 percent — that represents the academic standard for course progression. Students learn to calibrate their preparation effort toward this threshold: knowing what 75 percent accuracy feels like on nursing school exams, what content coverage produces it, and what preparation intensity is needed to reliably achieve it. When these students begin NCLEX preparation, they carry this accuracy calibration with them — and consistently experience early practice question accuracy of 50 to 58 percent as deeply concerning evidence of inadequate preparation.
Why This Gap Matters for NCLEX Preparation
The accuracy standard the NCLEX uses to determine passing is completely different from nursing school passing thresholds — and nursing school does not always explicitly teach this difference. The NCLEX does not pass candidates who answer a specific percentage of questions correctly. It passes candidates whose overall response pattern places their clinical reasoning ability estimate above the passing standard — a standard that corresponds to approximately 55 to 60 percent accuracy on a well-calibrated question bank presenting mixed-difficulty questions at the examination’s adaptive difficulty level. A nursing student who has spent three years calibrating preparation effort toward 75 to 80 percent accuracy discovers that 57 percent practice accuracy on a quality NCLEX preparation question bank feels like failing when it is actually at or approaching readiness. This calibration error produces anxiety that impairs preparation quality, produces unnecessary extension of preparation beyond benchmark confirmation, and produces vulnerability to switching to lower-difficulty question banks that produce higher accuracy numbers but lower examination readiness. NCLEX preparation must explicitly recalibrate the accuracy expectation from nursing school standards to the 55 to 60 percent NCLEX-specific threshold.
Gap 3: The Adaptive Testing Format and What It Means During the Exam
What Nursing School Teaches
Nursing school examinations are fixed-format assessments: a defined number of questions at a relatively consistent difficulty level, administered to all students in a cohort, with a percentage correct determining the result. Students develop a consistent relationship between the subjective experience of exam difficulty and their likely performance — if the exam felt hard, performance may be lower; if it felt manageable, performance is likely higher. This relationship between subjective difficulty experience and performance outcome is a reasonable heuristic for fixed-format examinations. It is completely unreliable for the NCLEX’s computerized adaptive format.
Why This Gap Matters for NCLEX Preparation
The NCLEX’s adaptive format inverts the subjective difficulty-to-performance relationship that nursing school has trained students to rely on. The CAT algorithm selects progressively harder questions for candidates whose ability estimate rises above the passing standard — meaning a candidate performing well will experience the exam as getting harder, not easier. A candidate whose exam feels hard throughout may be performing excellently (the algorithm is tracking a high ability estimate) or poorly (the algorithm has determined the ability is below the passing standard and is confirming it). Exam difficulty experience is not a reliable performance signal in either direction. NCLEX preparation must explicitly teach this counterintuitive relationship before exam day — because candidates who discover it for the first time during the actual examination will interpret a hard mid-exam experience as evidence of poor performance, which generates anxiety that degrades the clinical reasoning quality that was actually producing the difficulty increase. Understanding the adaptive format before sitting the exam protects against this self-undermining mid-exam anxiety spiral.
Gap 4: Therapeutic Communication as a Technical Skill

What Nursing School Teaches
Nursing school teaches communication in the context of clinical practice — how to build therapeutic relationships, how to conduct patient assessments through effective interviewing, how to deliver difficult information with compassion and clarity. These communication skills are genuinely important for nursing practice. They are taught, appropriately, as context-dependent skills that require professional judgment in their application — the right communication approach depends on the patient, the clinical situation, the relationship, and the therapeutic goals of the interaction.
Why This Gap Matters for NCLEX Preparation
The NCLEX tests therapeutic communication as a technical skill with specific named techniques that produce correct answers and specific named non-therapeutic responses that produce incorrect answers — regardless of how warm, empathic, or contextually reasonable the non-therapeutic response might be in a real clinical interaction. Nursing students who approach therapeutic communication questions through the clinical judgment and contextual sensitivity that nursing school appropriately teaches will consistently select options that sound nursing-appropriate in real-world practice but fail the NCLEX’s specific technique criteria. Open-ended questioning, reflection, clarification, focusing, and silence are the five therapeutic techniques that most commonly produce correct NCLEX answers. False reassurance, advice-giving, changing the subject, minimizing, and defending the institution are the five non-therapeutic responses that most commonly produce attractive but incorrect distractors. NCLEX preparation must teach these as a technical taxonomy — not because real nursing communication is that simple but because the examination tests a specific, named framework that context-dependent judgment alone does not reliably apply.
Gap 5: The Nursing Process as an NCLEX Answer Framework
What Nursing School Teaches
Nursing school teaches the nursing process — assessment, diagnosis, planning, implementation, evaluation — as a clinical practice framework for organizing nursing care. Students learn to apply it in clinical rotations, in care plan assignments, and in clinical reasoning exercises as a systematic approach to patient care. The nursing process as taught in nursing school is an iterative, cyclical framework that nurses use continuously and often simultaneously across its stages — a nurse assessing a patient is often simultaneously implementing prior plan elements and evaluating previous interventions.
Why This Gap Matters for NCLEX Preparation
The NCLEX tests the nursing process as a sequential answer framework for what-does-the-nurse-do-first questions — not as a clinical practice model that is applied iteratively and simultaneously. When the NCLEX asks what the nurse does first in a clinical scenario that presents multiple possible actions, the correct answer almost always reflects the nursing process sequence: assessment comes before diagnosis, diagnosis before planning, planning before implementation. The assessment-before-intervention principle — selecting the assessment option before the intervention option when both appear as choices and the stem has not already established that the relevant assessment is complete — is one of the most consistently tested NCLEX answer patterns across all clinical content areas. Nursing school teaches the nursing process as a practice framework. NCLEX preparation must additionally teach it as a sequential tiebreaker for first-action questions — a different and more mechanical application than the iterative clinical practice model nursing school appropriately emphasizes.
Gap 6: The NGN Clinical Judgment Framework
What Nursing School Teaches
Nursing school curricula published before 2023 rarely include explicit instruction on the NCSBN’s Clinical Judgment Measurement Model — the six-skill framework (recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, evaluate outcomes) that governs the Next Generation NCLEX question design. Even programs that have incorporated CJMM elements since the 2023 NGN launch vary significantly in how explicitly and how extensively they teach the framework and its mapping to specific NGN question format types. Most nursing students encounter the CJMM for the first time in NCLEX preparation rather than in nursing school — which means that NGN format questions feel structurally arbitrary without the framework that makes them intelligible.
Why This Gap Matters for NCLEX Preparation
Without explicit CJMM framework instruction, NGN NCLEX questions feel like a harder version of traditional multiple choice — more options, more complexity, more confusion — rather than what they actually are: structured assessments of six specific, named, individually practicable cognitive skills. A nursing student who does not know that a question asking them to identify the most significant clinical findings is testing the recognize cues skill, that a question asking them to explain what those findings indicate is testing the analyze cues skill, and that a question asking them to rank clinical explanations by urgency is testing the prioritize hypotheses skill approaches all three questions with the same general clinical reasoning strategy — which works for some and fails for others in ways that are difficult to understand or correct. NCLEX preparation must begin with explicit CJMM framework instruction — studying the NCSBN official documentation at ncsbn.org — before any NGN format practice, because the framework converts the format from opaque to systematic.
Gap 7: Error Type Classification as a Study Tool
What Nursing School Teaches
Nursing school teaches students to review incorrect exam answers through the lens of what clinical content they need to know better — which units to re-read, which concepts to revisit, which professor’s notes to review more carefully. This content-focused review approach is appropriate for nursing school examinations that primarily test content recall and recognition. The implicit assumption behind it — that incorrect answers reveal content that needs more study — is a reasonable assumption for examinations designed to test content.
Why This Gap Matters for NCLEX Preparation
For NCLEX preparation, the content-focused review assumption is accurate for only one of four error types — the knowledge gap, where the clinical principle genuinely required for the correct answer was absent from the accessible knowledge base. The other three error types — reasoning pattern error, patient context error, and NGN cognitive skill error — require different interventions than content review, and applying content review to them produces preparation effort without preparation improvement. Nursing students who learned to review incorrect answers by returning to content will default to this approach for every NCLEX incorrect answer — which means reasoning pattern errors (the most common incorrect answer type) will be treated with content review that cannot correct them, producing the frustrating experience of re-reading content that was already understood and still missing the same type of question on subsequent practice. NCLEX preparation must explicitly teach the four-category error type classification as a study tool — classifying every incorrect answer by error type before deciding on any preparation response is the foundation of efficient NCLEX preparation that nursing school’s content-review approach does not develop.
Gap 8: The Proceed Decision Is Data-Based, Not Feeling-Based
What Nursing School Teaches
Nursing school examinations have defined dates that all students sit simultaneously — the decision about when to take the exam is not a student’s individual choice but a faculty-determined schedule. Students develop no framework for making the personal proceed decision about when their preparation is sufficient for an examination they schedule themselves, because nursing school does not require that decision.
Why This Gap Matters for NCLEX Preparation
The NCLEX proceed decision — when to schedule and sit the examination — is one of the most consequential individual decisions in the entire preparation process, and nursing school provides no framework for making it. Without a framework, most nursing students default to feeling-based timing: sitting the exam when they feel ready (which, as earlier sections of this guide note, is a systematically unreliable readiness signal) or when anxiety about waiting becomes greater than anxiety about proceeding. Both feeling-based timing approaches produce worse outcomes than the data-based four-benchmark framework: proceed when overall accuracy is above 55 to 60 percent across at least 1,500 completed questions with upward trend, when no content category is below 50 percent in the most recent simulation, when NGN accuracy is above 50 percent tracked separately, and when a passing-range full simulation has been completed within two weeks of the target exam date. NCLEX preparation must explicitly teach this framework and the habit of making exam date decisions based on benchmark data rather than subjective readiness assessment, because nursing school has not provided any equivalent framework for the proceed decision that the NCLEX uniquely requires.
- The most important single thing nursing school could teach about the NCLEX that it often doesn’t: The explicit three-tier priority hierarchy — ABCs, then Maslow physiological and safety needs, then nursing process sequence — applied as an automatic pre-option sequence before every priority question. This framework, once automatic, improves accuracy across every clinical content area simultaneously. It takes approximately two weeks of deliberate practice to build to automaticity. It is the single preparation investment with the highest cross-content return in any NCLEX preparation period.
- How to use nursing school content knowledge most efficiently in NCLEX preparation: Nursing school content knowledge is the raw material that the NCLEX’s clinical reasoning frameworks process into correct answers. The most efficient use of that content knowledge in NCLEX preparation is not reviewing it again but applying it to novel clinical scenarios through the explicit frameworks this guide describes — the three-tier hierarchy for priority questions, the therapeutic communication technique taxonomy for communication questions, the nursing process sequence for first-action questions, and the CJMM cognitive skill framework for NGN format questions. Framework application practice produces more NCLEX accuracy improvement per hour than content review for candidates whose primary preparation gap is framework application rather than content knowledge.
- What to tell nursing students still in school who are reading this: Begin 10 to 25 NCLEX-style practice questions per day on a quality question bank now — not at a volume that competes with nursing school demands, but enough to begin encountering the NCLEX’s specific reasoning frameworks in the question format that the exam uses. Every week of exposure to NCLEX-style questions while in nursing school builds the question-reading habits, framework application instincts, and clinical reasoning patterns that post-graduation intensive preparation then accelerates rather than builds from zero. The most efficient NCLEX preparation timeline begins during nursing school, not after graduation.
Conclusion
Nursing school provides an excellent clinical foundation — the content knowledge, clinical experience, and professional values that NCLEX preparation builds on. What it does not always provide explicitly is the specific reasoning architecture the NCLEX uses to test that foundation: the three-tier priority framework that organizes every priority answer, the 55 to 60 percent accuracy calibration that correctly interprets practice performance, the adaptive format understanding that prevents mid-exam performance anxiety, the therapeutic communication technical taxonomy that produces correct communication answers, the nursing process sequential application that answers first-action questions, the CJMM six-skill framework that makes NGN format questions intelligible, the error type classification that identifies the correct preparation response to each incorrect answer, and the benchmark proceed decision framework that makes the exam timing decision on data rather than feeling.
These eight gaps are not evidence that nursing school has failed. They are the specific translation layer between excellent nursing education and NCLEX-ready clinical reasoning — and filling them is exactly what NCLEX preparation is for. Candidates who understand these gaps before beginning preparation fill them efficiently and directly. Candidates who discover them mid-preparation through frustrated practice session experiences fill them more slowly and with more anxiety than necessary. This guide exists to produce the former experience rather than the latter.