NCLEX flashcards are one of the most widely used and most widely misused preparation tools available to nursing candidates. The problem is not with flashcards themselves — the retrieval practice mechanism they employ is one of the most robustly supported memory consolidation methods in cognitive psychology. The problem is with how most candidates design and use them. A card that asks What are the signs of hypokalemia? and answers potassium below 3.5, muscle weakness, cramps, dysrhythmias is testing list recognition rather than clinical reasoning. A card that presents a clinical scenario and asks the candidate to identify the priority nursing action, explain why it is the priority, and name the distractor type that would lead a candidate to the wrong answer is building the clinical judgment that the NCLEX actually measures.
Most pre-made NCLEX flashcard decks are built on the recognition model. They are organized around content categories, present facts as the primary unit of study, and are designed to be reviewed until the candidate recognizes the correct answer reliably when shown. Recognition without retrievability is the fluency illusion — the clinical content feels well-known during review because it is familiar, but when a novel NCLEX question presents the same content in an unfamiliar clinical scenario, the familiar pattern is absent and the knowledge is not accessible. The candidates who benefit most from NCLEX flashcards are not those who review them most frequently but those who build them most deliberately — from clinical reasoning gaps identified through practice question rationale review rather than from generic content lists. This guide provides the complete NCLEX flashcard strategy: the design principles that distinguish clinical reasoning cards from content recognition cards, the five high-yield card categories that produce the most exam-relevant retrieval practice, the card creation workflow that sources cards from documented preparation gaps rather than from content coverage checklists, the review protocols that maximize retention from each review session, how to combine digital and physical cards for different preparation functions, and the most common flashcard mistakes that reduce their preparation value regardless of card quantity.
Why Most NCLEX Flashcards Fail — and What Actually Works
Understanding the specific design failures that limit most NCLEX flashcards prepares candidates to make deliberate, evidence-based choices about how to build their own and how to evaluate pre-made decks.
The Recognition vs. Retrieval Distinction
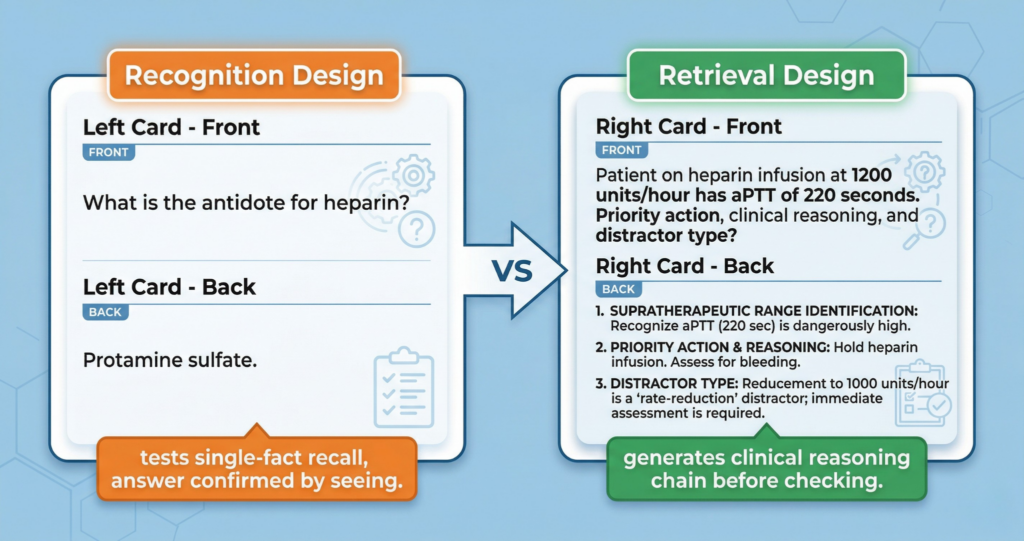
The fundamental failure of most NCLEX flashcards is designing for recognition rather than retrieval. Recognition is the ability to identify the correct answer when it is presented — as it is on the front of a flashcard showing the question with the back available to confirm. Retrieval is the ability to generate the correct answer from memory without any presented options or cues — as the NCLEX requires when clinical reasoning must produce the correct action from scenario data alone. These two cognitive processes use different memory mechanisms and produce different levels of encoding durability. Cards that present a cue-answer pair and require the reviewer to recognize the answer upon seeing the cue build recognition memory. Cards that present a clinical scenario requiring the reviewer to generate a complete clinical response from memory before checking the answer back build retrieval memory. Recognition is fast and feels productive during review; retrieval is effortful and uncomfortable. The discomfort of genuine retrieval is the preparation signal — it means the memory reconstruction is occurring, which is the mechanism that produces durable encoding. NCLEX flashcards designed to feel comfortable during review are not producing the retrieval effort that makes preparation effective.
The Atomization Problem
The atomization problem describes the tendency to build NCLEX flashcards around isolated clinical facts rather than around clinical reasoning chains. An atomized card tests: What is the antidote for heparin? Protamine sulfate. A reasoning chain card tests: A patient receives a heparin infusion at 1,200 units/hour after coronary stent placement. Two hours later the aPTT is 220 seconds. What is the nurse’s priority, and what distinguishes this clinical finding from therapeutic anticoagulation? The atomized card produces a single retrievable fact. The reasoning chain card produces a clinical reasoning process — identifying aPTT supratherapeutic range (60 to 100 seconds is therapeutic), recognizing this as anticoagulant overdose, identifying the priority of holding the heparin infusion and assessing for bleeding while notifying the provider, and naming the distractor of simply reducing the rate. Atomized NCLEX flashcards can be created quickly and reviewed quickly — but they produce a knowledge base that cannot be flexibly applied to novel clinical scenarios. Reasoning chain cards take longer to create and review but produce the clinical reasoning competency the exam measures.
The Quantity Trap
The quantity trap in NCLEX flashcards is the belief that a larger deck produces better preparation — that 2,000 cards is better than 500 cards because more content is covered. This belief fails for two reasons. First, a large deck of atomized recognition cards covers more content but builds less clinical reasoning than a small deck of high-quality reasoning chain cards. Second, large decks produce unsustainable daily review volumes that cause system abandonment — the preparation tool with the highest theoretical value becomes the one least consistently used. The most effective NCLEX flashcard systems have 150 to 400 cards built entirely from documented preparation gaps: clinical principles that were wrong, unclear, or reasoning-pattern failures that practice session rationale review identified. Each card in this precision deck represents a specific gap that needs to be closed. A 300-card precision deck reviewed daily at the optimal intervals closes 300 specific preparation gaps. A 2,000-card coverage deck reviewed sporadically when time allows closes far fewer because the review cadence never reaches the intervals that produce durable encoding.
The Five High-Yield NCLEX Flashcard Categories

Rather than organizing NCLEX flashcards by body system or content category — which produces encyclopedic coverage decks — the most preparation-efficient organization focuses on the five card types that generate the highest clinical reasoning development per review minute.
Category 1: Pharmacology Safety Chain Cards
Pharmacology safety chain cards are the single highest-yield NCLEX flashcard category because pharmacology questions appear across all content areas and consistently require the specific nursing assessment-action-monitoring chain that generic drug fact cards do not develop. Each pharmacology safety chain card presents a clinical scenario involving a specific drug class — not the drug name in isolation — with a patient context that requires clinical judgment: a patient receiving digoxin reports nausea and visual disturbances, potassium is 2.9; a patient on lithium reports polyuria and fine hand tremor; a patient receiving magnesium sulfate for pre-eclampsia has a respiratory rate of 10. The back of each card contains the complete safety chain: what the finding indicates clinically (early toxicity signs for each drug), which assessment parameter confirms the severity (digoxin level, lithium level, deep tendon reflexes for magnesium), what the immediate nursing action is (hold the medication, notify provider, specific monitoring), and what distractor type a candidate typically selects instead (continuing administration with increased monitoring, adjusting the dose). Pharmacology safety chain cards build the complete clinical reasoning architecture that the NCLEX tests in medication questions, not just the facts that support pattern recognition.
Category 2: Priority Clinical Decision Cards
Priority clinical decision cards present clinical scenarios with competing priorities and require the candidate to generate the correct priority choice, the framework that justifies it, and the reasoning error that would produce the wrong choice. A post-operative patient has pain rated 8 out of 10, oxygen saturation of 88 percent, and is requesting to call their family — what is the priority and which framework applies? A patient in the medical ICU has been speaking clearly for the past hour but now has a Glasgow Coma Scale score of 12 and is increasingly restless — what does the nurse do first and why? These NCLEX flashcards build the priority reasoning skill that is tested more consistently than any other clinical judgment on the exam. The front presents the clinical scenario with competing priorities. The back provides the tier-by-tier priority analysis: which finding represents the ABC threat or highest-urgency physiological need, which framework governs the decision, and what the most compelling wrong-choice distractor represents in priority framework terms.
Category 3: Assessment Finding Significance Cards
Assessment finding significance cards present a clinical finding in context and require the candidate to generate its clinical significance — what it indicates, what it requires the nurse to do immediately, and what would happen if it were missed or misinterpreted. A patient 24 hours post-thyroid surgery reports tingling around the mouth and fingertip numbness — what does this indicate, what assessment confirms it, and what is the immediate nursing response? A post-cardiac surgery patient’s mediastinal drainage tube suddenly stops producing output after producing 150 mL per hour — what does this indicate and what is the nursing priority? These NCLEX flashcards develop the clinical recognition skill that distinguishes nursing from mere task execution — the ability to interpret the significance of clinical data rather than only respond to explicit clinical orders. The back of each card provides the finding interpretation, the confirming assessment, the priority nursing action, and the consequence of missed recognition.
Category 4: Therapeutic Communication Discrimination Cards
Therapeutic communication discrimination cards present patient statements alongside three to four nurse responses and require the candidate to identify which response is therapeutic and explain specifically why each other response is not. A patient says I do not know why I am even in this hospital, nothing is going to get better — followed by four nurse responses including an open-ended facilitation, a false reassurance, a topic change, and a reflective response. The card requires generating which is therapeutic and naming the specific technique failure in each non-therapeutic option. These NCLEX flashcards build the therapeutic communication discrimination that practice questions alone develop slowly — by creating explicit language for the technique failures in non-therapeutic responses (this is false reassurance because it closes communication by invalidating the patient’s concern, this is topic change because it withdraws therapeutic presence at the moment it is most needed), the cards make the distinctions visible and retrievable in ways that simply practicing communication questions does not.
Category 5: Pathophysiology-to-Nursing-Action Chain Cards
Pathophysiology-to-nursing-action chain cards connect clinical findings to their underlying mechanisms and then to the nursing actions those mechanisms require — building the mechanistic understanding that makes clinical nursing knowledge derivable rather than memorized. A patient with left-sided heart failure has crackles, dyspnea, and oxygen saturation of 89 percent — trace the physiological chain from the mechanism to the clinical findings to the nursing priorities and explain why each intervention addresses a specific element of the mechanism. These NCLEX flashcards produce the most durable clinical knowledge because mechanistically understood content is retrievable from multiple starting points — from the finding, from the mechanism, or from the nursing action — rather than only from the specific cue the card originally presents. A candidate who has built pathophysiology-to-nursing-action chain cards for heart failure can answer any heart failure question regardless of which element of the clinical picture the question emphasizes.
Review Protocols That Maximize Retention From Every Session
Card design determines the quality of what is being reviewed. Review protocol determines how effectively each review session converts card exposure into durable clinical reasoning. Both dimensions must be optimized — high-quality cards reviewed passively produce less retention than they should; even low-quality cards reviewed actively produce more retention than passive review would.
The Generate-Before-Flip Discipline
The generate-before-flip discipline is the foundational active review protocol for all NCLEX flashcards. Before the answer side of any card is revealed, generate the complete clinical response from the scenario prompt from memory — the clinical principle, the priority nursing action, the distractor identification — and hold it in working memory or write it briefly. Then flip the card and compare. This comparison is the learning event: when generated content matches the card back, the retrieval was successful and consolidation occurred. When generated content is incomplete or incorrect, the gap between what was generated and what the card back shows is the specific encoding failure that the next review will address. The generate-before-flip discipline requires more time and more cognitive effort per card than reading-and-confirming review. It also produces three to five times more durable memory encoding for the same number of cards reviewed. The discomfort and slowness of genuine generation are the signals that the most valuable review events are occurring.
The Oral Explanation Review
The oral explanation review is a NCLEX flashcards review protocol that builds the clinical reasoning articulation that the NCLEX clinical judgment formats require. After generating the card back content, explain it aloud — as if teaching a nursing student — before moving to the next card. This additional step requires not just retrieving the content but organizing it into a coherent clinical explanation that connects the mechanism to the finding to the nursing action to the distractor logic. Oral explanation activates additional encoding pathways beyond the silent retrieval that standard generate-before-flip uses — the act of explaining requires the candidate to organize the clinical reasoning into a sequence that makes logical sense, which produces encoding at a deeper level of processing than retrieval alone. Cards that can be generated silently but stumble when explained aloud reveal reasoning chains that are recognizable but not fully organized — which is exactly the gap between practice question performance and actual exam performance for many candidates.
Triage Review: High-Value vs. Maintenance Cards
As the NCLEX flashcard deck matures across the preparation period, cards naturally stratify into two populations: high-value cards — those consistently answered incorrectly or with low confidence — and maintenance cards — those consistently answered correctly and confidently. High-value cards are the clinical reasoning gaps the deck was designed to close; they deserve full generate-before-flip plus oral explanation review at every scheduled appearance. Maintenance cards are gaps already closed; they deserve generate-before-flip at scheduled appearances to prevent decay without the additional oral explanation investment that already-mastered content no longer requires. In the final two weeks before the exam, concentrating the most intensive review resources on high-value cards — while maintenance cards receive standard interval review — produces the most efficient use of limited pre-exam preparation time. Never skip maintenance cards entirely: decay of previously mastered content is a real risk that the spaced repetition schedule prevents when followed consistently.
Digital vs. Physical NCLEX Flashcards: When to Use Each
Digital and physical NCLEX flashcards serve different preparation functions and are most effectively used in complementary roles rather than as direct substitutes for each other.
Digital Cards: Spaced Repetition and Mobile Review
Digital NCLEX flashcards in a spaced repetition application — primarily Anki — are the optimal format for the daily review session that maintains the spaced intervals that produce maximum consolidation efficiency. The algorithm tracks each card’s performance history, calculates the optimal review interval, and surfaces each card at the moment when retrieval requires effortful reconstruction rather than immediate access. This algorithmic scheduling is impossible to replicate with physical cards at the same precision — which is why digital NCLEX flashcards in a spaced repetition system produce more durable retention per review hour than equivalent physical card review. Digital cards are also the optimal format for mobile fragmented-time review: a 15-minute commute, a lunch break, or any available window of 10 or more minutes can contribute meaningful review sessions without carrying physical materials. The digital format is the primary delivery mechanism for the daily maintenance review that prevents decay across the preparation period.
Physical Cards: Active Creation and Deep Processing
Physical NCLEX flashcards serve a preparation function that digital cards cannot replicate: the act of handwriting a card produces a deeper initial encoding than typing the same content. The physical act of writing a clinical principle by hand activates motor and spatial memory in addition to semantic memory — producing a multi-pathway initial encoding that is more resistant to early forgetting than typed encoding alone. Physical cards are most valuable at the creation stage: writing the clinical scenario on the front and the three-component clinical reasoning chain on the back by hand produces a more thorough initial encoding of the card content than digital card creation. These handwritten cards can then be photographed and entered into the digital spaced repetition system for ongoing review, combining the encoding benefits of physical creation with the scheduling benefits of digital review. Physical cards also provide a tactile, screen-free review option that some candidates find maintains engagement when digital screen fatigue sets in during long preparation sessions.
Recommended Hybrid Implementation
The most effective NCLEX flashcard implementation for most candidates is a hybrid approach: create cards by hand using the five high-yield category format and three-component back structure, enter them into Anki within 24 hours for digital spaced repetition scheduling, and use digital review for the daily morning session and mobile fragmented-time review. Reserve physical card review for the Saturday deep session context review — spreading relevant physical cards for a content area alongside practice questions in the same area to make the clinical connections between card content and question application visible in a physical spatial arrangement that digital review cannot replicate. This hybrid combines the encoding depth of physical creation, the scheduling precision of digital spaced repetition, and the connection visualization that physical card arrangement provides.
The Most Common NCLEX Flashcard Mistakes and How to Avoid Them
Even well-intentioned NCLEX flashcard strategies produce limited preparation value when specific implementation mistakes reduce the quality of the cards, the consistency of the review, or the cognitive engagement during review sessions.
Building Too Many Cards Too Quickly
Creating large numbers of NCLEX flashcards in short periods produces a review backlog that rapidly becomes overwhelming and causes system abandonment. Five to eight new cards created per study session — from documented gaps identified during that session’s rationale review — produces a sustainable review volume that never exceeds 30 to 40 due cards per daily review session. Creating 30 to 50 new cards during a content review marathon produces a review burden within two weeks that exceeds most candidates’ daily time availability. The daily new card limit is not a suggestion but a preparation system protection: exceeding it consistently ensures that the system will eventually collapse under its own review burden. When a particularly productive content review session generates 20 card-worthy principles, record them all in a dedicated note and create five to eight per day from that list across the following days rather than entering all 20 simultaneously.
Passive Recognition Review
The most common NCLEX flashcard review mistake is reading the front and then immediately flipping to the back without any genuine retrieval attempt — processing the card as a reading exercise rather than a retrieval exercise. This passive recognition review feels like studying and produces almost none of the memory consolidation benefit that retrieval practice generates. The card reviewer who reads a clinical scenario, immediately flips to confirm the answer, nods, and moves to the next card is building familiarity without durability — which is the fluency illusion that collapses under novel exam question presentations. The generate-before-flip discipline is non-negotiable: no card is flipped before a genuine retrieval attempt has been made, however incomplete or uncertain. An incomplete retrieval attempt followed by full back-of-card review is the most valuable review interaction in the system; a complete skip to the answer is the least valuable.
Using Cards as a Substitute for Question Practice
NCLEX flashcards build clinical content consolidation and reasoning principle retention — they do not build the clinical scenario reasoning practice that question bank sessions develop. Candidates who replace question bank sessions with extended flashcard review sessions are building knowledge retention without the clinical reasoning application practice that the exam tests. A preparation day that includes 60 minutes of flashcard review and zero practice questions produces less clinical reasoning development than a day with 20 minutes of flashcard review and 40 minutes of practice questions with rationale review. NCLEX flashcards are most effective in the first 20 to 30 minutes of a preparation session — activating clinical reasoning associations before the primary question bank session rather than replacing it. Keep the time allocation proportionate: flashcard review is a consolidation supplement, not a clinical reasoning development substitute.
- Common mistake: Reviewing cards in the same order every time. Fixed-order review converts retrieval practice into pattern recognition — the card that always follows card A generates pre-recognition that reduces the retrieval effort the spacing effect requires. Use random order shuffling in every review session to maintain genuine retrieval demands.
- Common mistake: Creating cards from content that is already mastered. The card creation trigger is the transfer question — does this change how I reason about similar scenarios? If the clinical principle is already consolidated, a card is not needed and creates unnecessary review burden. New cards are for gaps, not for coverage.
- Common mistake: Abandoning the deck in the final two weeks before the exam. The final two weeks are when long-interval review cards reach their scheduled due dates — the consolidation reviews that convert recent learning into durable long-term memory. Maintaining the daily review through exam week at a reduced but consistent volume preserves this consolidation rather than allowing the final weeks of preparation to decay.
Conclusion
NCLEX flashcards are a clinical reasoning development tool when designed around five high-yield category formats — pharmacology safety chains, priority clinical decisions, assessment finding significance, therapeutic communication discrimination, and pathophysiology-to-nursing-action chains — and built from documented preparation gaps identified through practice question rationale review. They are a content recognition tool when built from generic content lists and reviewed passively. The design distinction determines which type of clinical reasoning the card builds; the review protocol determines whether that clinical reasoning becomes durably encoded.
The generate-before-flip discipline converts every card review into a retrieval practice event. The oral explanation review builds the reasoning articulation that the NCLEX clinical judgment formats test. The rationale-to-card pipeline ensures every card represents a specific gap that needs to be closed. The daily five-to-eight card creation limit prevents the review backlog that collapses most card systems. The hybrid digital-physical approach combines the encoding depth of handwritten creation with the scheduling precision of algorithmic spaced repetition. Build NCLEX flashcards from gaps, review them actively, and maintain the daily review through exam week — and the clinical reasoning library that accumulates across the preparation period arrives at exam day in the maximum retrieval-ready state that any preparation method can produce.