NCLEX medical surgical nursing is the broadest and most heavily weighted content category on the exam. Physiological integrity — the overarching test plan category that encompasses medical-surgical content — accounts for approximately 38 to 62 percent of the NCLEX-RN in 2026, making it the single largest preparation target by a significant margin. A candidate who performs well in NCLEX medical surgical nursing has a substantial preparation advantage regardless of performance in other content areas. A candidate with significant gaps in this category cannot compensate for them through strength in lower-weighted areas.
The challenge with NCLEX medical surgical nursing is not the breadth of topics — every body system is represented, from cardiovascular and respiratory to neurological, renal, endocrine, gastrointestinal, and musculoskeletal. The challenge is knowing which concepts within each system the NCLEX actually tests, at what cognitive level, and in what clinical scenario contexts. A candidate who studies every detail of every body system at equal depth will spend preparation time inefficiently and likely still have gaps in the highest-yield areas. A candidate who understands which NCLEX medical surgical nursing topics appear most consistently, what clinical reasoning the questions test, and how priority assessment and intervention principles apply across systems will perform consistently above the passing standard.
This guide covers the highest-yield NCLEX medical surgical nursing topics across the six most heavily tested body systems: cardiovascular, respiratory, neurological, renal, endocrine, and gastrointestinal. For each system, the focus is on the specific conditions, clinical presentations, assessment priorities, and nursing interventions that appear most consistently on the exam — not encyclopedic coverage but the precise clinical knowledge and reasoning applications that the CAT algorithm targets at the passing standard level and above.
Cardiovascular Nursing: The Highest-Yield Med-Surg System
Cardiovascular nursing is the single most consistently tested topic within NCLEX medical surgical nursing. Heart failure, acute coronary syndrome, dysrhythmias, and peripheral vascular disease appear across all difficulty levels and in both standalone questions and NGN unfolding case study formats.
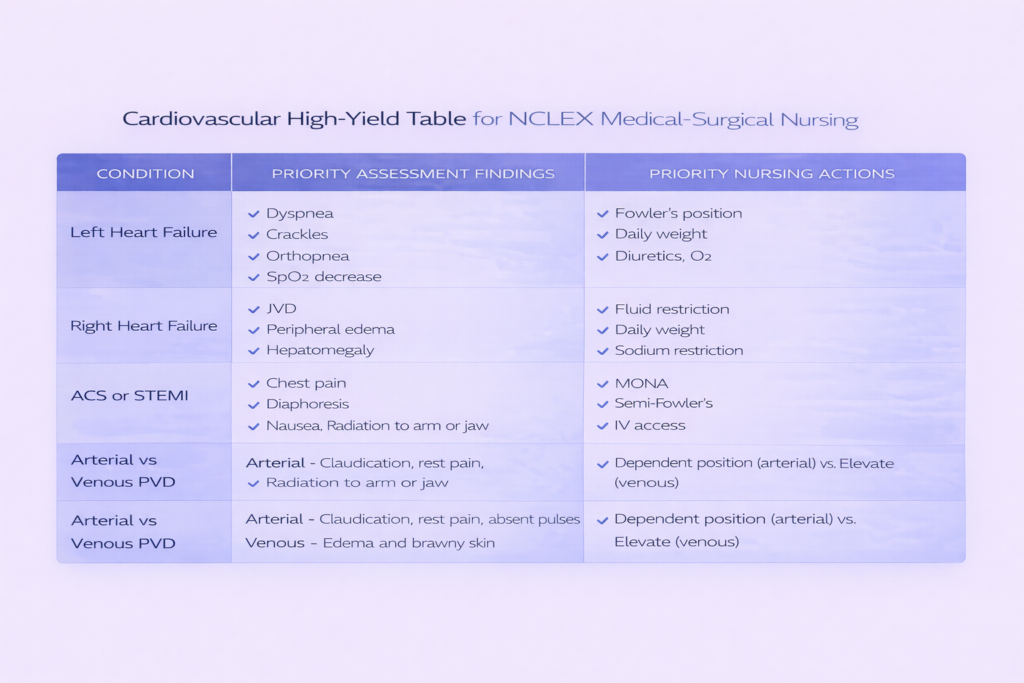
Heart Failure: Left vs. Right Sided
Heart failure questions in NCLEX medical surgical nursing consistently test whether candidates can distinguish left-sided from right-sided failure by their clinical manifestations and apply the correct priority assessment and interventions for each. Left-sided heart failure impairs forward flow of blood from the left ventricle, causing fluid to back up into the pulmonary circulation — the result is pulmonary congestion presenting as dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, crackles in the lung bases, pink frothy sputum in severe cases, and decreased oxygen saturation. Right-sided heart failure impairs forward flow from the right ventricle, causing fluid to back up into the systemic venous circulation — the result is peripheral edema particularly in the ankles and sacrum for bedbound patients, jugular venous distension, hepatomegaly, and ascites. The most important NCLEX medical surgical nursing assessment rule for heart failure is that daily weight is the most sensitive early indicator of fluid retention — 1 kg of weight gain represents approximately 1 liter of fluid accumulation. A weight gain of more than 2 kg in 24 hours warrants provider notification and likely diuretic adjustment.
Acute Coronary Syndrome and STEMI
Acute coronary syndrome encompasses unstable angina, NSTEMI, and STEMI — the spectrum of conditions resulting from coronary artery occlusion or near-occlusion. NCLEX medical surgical nursing questions on ACS test priority assessment and the MONA mnemonic for initial management: Morphine for pain relief and anxiety reduction, Oxygen only if oxygen saturation falls below 94 percent (supplemental oxygen is no longer recommended routinely for ACS patients with normal saturation), Nitroglycerin for vasodilation and pain relief, and Aspirin for platelet aggregation inhibition. Position the patient in semi-Fowler’s, obtain a 12-lead ECG immediately, establish IV access, and prepare for possible percutaneous coronary intervention. The highest-priority NCLEX medical surgical nursing assessment finding in suspected MI is new-onset chest pain radiating to the left arm, jaw, or back — particularly when accompanied by diaphoresis, nausea, and shortness of breath. Female patients and diabetic patients may present with atypical MI symptoms including fatigue, nausea, and jaw or epigastric pain without classic chest pressure.
Cardiac Dysrhythmias: Priority Identification
Dysrhythmia recognition and priority response is a high-yield NCLEX medical surgical nursing topic tested across all difficulty levels. The most clinically dangerous dysrhythmias — ventricular fibrillation and pulseless ventricular tachycardia — require immediate defibrillation, and CPR should be initiated while the defibrillator is being prepared. Unstable ventricular tachycardia with a pulse requires synchronized cardioversion. Atrial fibrillation produces an irregularly irregular rhythm and carries high stroke risk from atrial thrombus formation — anticoagulation management and ventricular rate control are priority nursing concerns. Third-degree heart block (complete heart block) produces complete dissociation between atrial and ventricular conduction and requires temporary pacing and preparation for permanent pacemaker placement. The NCLEX medical surgical nursing clinical reasoning principle for dysrhythmias is always assess the patient before the monitor — a patient who is alert, talking, and hemodynamically stable tolerates a rhythm that appears threatening on the monitor better than the monitor alone suggests.
Peripheral Vascular Disease: Arterial vs. Venous
Peripheral vascular disease questions in NCLEX medical surgical nursing test whether candidates can distinguish arterial insufficiency from venous insufficiency by presentation and apply the correct position and wound care principles for each. Arterial insufficiency produces intermittent claudication, rest pain that worsens with elevation and improves with dependent positioning, pale or cyanotic cool extremities, absent or diminished pulses, and wounds that appear pale or necrotic without edema. Venous insufficiency produces chronic aching that worsens with dependency and improves with elevation, brown discoloration and brawny edema of the lower legs, and wounds with irregular edges and moderate drainage. The position rule is the most frequently tested distinction: elevate venous insufficiency extremities to reduce edema, and keep arterial insufficiency extremities at or below heart level to promote blood flow. Elevation of an arterially compromised extremity worsens ischemia — a critical NCLEX medical surgical nursing safety rule.
Respiratory Nursing: Airway First, Always
Respiratory nursing is the second highest-yield system in NCLEX medical surgical nursing. Airway and oxygenation are the top of the physiological priority hierarchy — any respiratory finding that threatens airway patency or adequate oxygenation takes priority over all other clinical concerns regardless of the scenario context.
COPD: The Hypoxic Drive Principle
COPD questions in NCLEX medical surgical nursing almost always test the hypoxic drive principle and its nursing implications. In patients with chronic CO2 retention from long-standing COPD, the normal hypercapnic respiratory drive is blunted and breathing is driven primarily by relative hypoxemia. Administering high-flow supplemental oxygen to these patients may eliminate the hypoxic drive and suppress respiratory effort, potentially causing respiratory depression. The NCLEX medical surgical nursing oxygen rule for COPD is to target oxygen saturation of 88 to 92 percent rather than the normal 95 to 100 percent range, using low-flow oxygen delivery initially and titrating based on clinical response. This principle is tested as a priority action question — when a patient with known COPD is in respiratory distress, the oxygen delivery method and target saturation, not simply applying the highest available flow rate, determines the correct answer.
Pneumonia: Assessment and Aspiration Risk
Pneumonia questions in NCLEX medical surgical nursing test assessment findings, priority interventions, and aspiration precautions. The classic assessment findings include fever, productive cough with purulent or rust-colored sputum, crackles and diminished breath sounds over the affected lobe, pleuritic chest pain, and elevated white blood cell count. Priority nursing interventions include positioning the patient with the affected lung uppermost to promote drainage, encouraging deep breathing and coughing, maintaining adequate hydration to liquefy secretions, and administering ordered antibiotics within the prescribed timeframe. For patients at high aspiration risk — those with dysphagia, altered level of consciousness, or receiving enteral feedings — elevating the head of bed to 30 to 45 degrees and keeping it elevated for 30 to 60 minutes after feedings are the key NCLEX medical surgical nursing aspiration prevention interventions.
Pulmonary Embolism: Recognition and Emergency Response
Pulmonary embolism is a high-acuity NCLEX medical surgical nursing topic that tests recognition of sudden respiratory deterioration in a high-risk patient. The classic PE presentation includes sudden onset dyspnea, pleuritic chest pain, tachycardia, and tachypnea — frequently in a patient with known risk factors such as prolonged immobility, recent surgery, lower extremity deep vein thrombosis, oral contraceptive use, or malignancy. The classic triad of dyspnea, chest pain, and hemoptysis occurs in a minority of cases but is highly specific when present. The NCLEX medical surgical nursing priority nursing action for a suspected PE is immediate provider notification while positioning the patient upright, applying supplemental oxygen, and preparing for diagnostic imaging and anticoagulation therapy. Anticoagulation — not thrombolytics — is the first-line treatment for most PE cases, with thrombolytics reserved for massive PE with hemodynamic instability.
Pneumothorax: Tension vs. Simple
Pneumothorax questions in NCLEX medical surgical nursing test the distinction between simple pneumothorax and tension pneumothorax and the emergency intervention required for each. Simple pneumothorax presents with unilateral diminished or absent breath sounds, chest pain, and mild respiratory distress — managed with chest tube insertion and water seal drainage. Tension pneumothorax is a life-threatening emergency presenting with severe respiratory distress, tracheal deviation away from the affected side, absent breath sounds, hypotension, distended neck veins, and cyanosis — requiring immediate needle decompression at the second intercostal space at the midclavicular line before chest tube insertion. The NCLEX medical surgical nursing tracheal deviation rule is critical: tracheal deviation toward the affected side suggests atelectasis or lung collapse; deviation away from the affected side indicates tension pneumothorax with mediastinal shift — an immediately life-threatening emergency.
Neurological Nursing: Assessment Precision and Emergency Recognition

Neurological nursing in NCLEX medical surgical nursing tests the ability to recognize acute neurological changes that signal emergencies, apply the correct monitoring sequence, and identify the specific nursing actions that prevent secondary injury.
Stroke: FAST Recognition and Time-Critical Intervention
Stroke questions in NCLEX medical surgical nursing test FAST recognition — Face drooping, Arm weakness, Speech difficulty, Time to call — and the time-critical intervention sequence. Ischemic stroke accounts for approximately 87 percent of all strokes and is potentially treatable with IV tissue plasminogen activator (tPA) within 3 to 4.5 hours of symptom onset, or with mechanical thrombectomy within a longer window for large vessel occlusions. The most important NCLEX medical surgical nursing rule for stroke is that thrombolytic therapy is contraindicated in hemorrhagic stroke — which must be ruled out by CT scan before tPA administration. The nursing priority before tPA is obtaining blood pressure — tPA is contraindicated if systolic BP is above 185 mmHg or diastolic above 110 mmHg at the time of administration, as uncontrolled hypertension significantly increases hemorrhagic transformation risk. Post-tPA nursing monitoring includes blood pressure every 15 minutes for the first 2 hours, then every 30 minutes for 6 hours, watching for signs of intracerebral hemorrhage: sudden severe headache, decreased level of consciousness, vomiting, and acute neurological deterioration.
Increased Intracranial Pressure: The Cushing Triad
Increased intracranial pressure is a neurological emergency tested consistently in NCLEX medical surgical nursing questions about TBI, stroke, hydrocephalus, and post-neurosurgical patients. The Cushing triad — the classic late sign of severely elevated ICP — consists of hypertension with a widening pulse pressure, bradycardia, and irregular respirations (Cheyne-Stokes pattern). The Cushing triad represents herniation in progress and requires immediate emergency intervention. Earlier signs of rising ICP that the NCLEX medical surgical nursing nurse should recognize and act on before the Cushing triad develops include decreasing level of consciousness, changes in pupillary response (unequal pupils, sluggish reaction), and headache worsening with position changes. Nursing interventions to reduce ICP include elevating the head of bed to 30 degrees in midline alignment — avoid hip flexion and head rotation which impair venous drainage — maintaining normothermia, controlling pain and agitation, and avoiding activities that increase intrathoracic pressure such as coughing, Valsalva, and suctioning beyond 10 seconds.
Spinal Cord Injury: Level-Specific Complications
Spinal cord injury questions in NCLEX medical surgical nursing test level-specific functional impairment and the life-threatening complication unique to cervical and high thoracic cord injury: autonomic dysreflexia. Autonomic dysreflexia occurs in patients with injuries at T6 or above and is triggered by a noxious stimulus below the level of injury — most commonly a distended bladder or bowel. It presents as a sudden severe hypertensive crisis accompanied by pounding headache, profuse diaphoresis and flushing above the injury level, pallor and piloerection below the injury level, and bradycardia. The NCLEX medical surgical nursing emergency response sequence is: sit the patient upright immediately to reduce blood pressure, identify and eliminate the triggering stimulus beginning with the bladder (check catheter patency, relieve retention), then bowel (check for impaction), then skin (check for pressure, tight clothing, or other irritation). Antihypertensive medication is administered if the trigger cannot be immediately identified or removed and blood pressure remains dangerously elevated.
Renal Nursing: Fluid Balance, Electrolytes, and Dialysis
Renal nursing in NCLEX medical surgical nursing tests fluid and electrolyte imbalances secondary to renal failure, the phases of acute kidney injury, chronic kidney disease dietary restrictions, and dialysis principles.
Acute Kidney Injury: Three Phases
Acute kidney injury questions in NCLEX medical surgical nursing test the three clinical phases and their distinct clinical presentations. The oliguric phase — the initial and most dangerous phase — is characterized by urine output below 400 mL per day, rising creatinine and BUN, hyperkalemia, metabolic acidosis, and fluid overload with edema and hypertension. The oliguric phase lasts days to weeks depending on severity and cause. The diuretic phase follows and is paradoxically dangerous despite improved urine output — the kidneys begin excreting large volumes of dilute urine (up to 5 liters or more per day) before tubular function is fully restored, creating risks of severe dehydration, hypokalemia, and hyponatremia from excessive fluid and electrolyte loss. The recovery phase involves gradual restoration of normal renal function over weeks to months. The NCLEX medical surgical nursing nursing priority shifts across phases: fluid restriction and hyperkalemia management during oliguria, fluid replacement and electrolyte monitoring during diuresis.
Chronic Kidney Disease: Dietary and Medication Restrictions
Chronic kidney disease questions in NCLEX medical surgical nursing consistently test dietary restrictions and medication implications. The CKD diet restricts potassium — avoid high-potassium foods such as bananas, oranges, potatoes, tomatoes, and salt substitutes that use potassium chloride; phosphorus — avoid dairy products, nuts, seeds, and processed foods with phosphate additives, and take phosphate binders with meals as ordered; sodium — to control blood pressure and fluid retention; and protein in early stages — to reduce the nitrogenous waste load the diseased kidneys must filter, though protein restriction is individualized and not universally applied. The NCLEX medical surgical nursing medication restriction in CKD is NSAIDs — ibuprofen, naproxen, and other NSAIDs reduce renal prostaglandin synthesis and can precipitate acute-on-chronic renal failure by causing renal vasoconstriction. Patients with CKD should be advised to avoid all NSAIDs for pain management.
Hemodialysis and Peritoneal Dialysis Nursing
Dialysis nursing questions in NCLEX medical surgical nursing test AV fistula care, dialysis complications, and post-dialysis assessment. For AV fistula care: never use the fistula arm for blood pressure measurement, IV insertion, or venipuncture; assess for bruit and thrill at each nursing assessment — absence indicates occlusion requiring immediate provider notification; avoid constricting clothing or positioning on the fistula arm. Post-hemodialysis assessment priorities include blood pressure monitoring for hypotension — the most common complication of hemodialysis — monitoring for disequilibrium syndrome in new dialysis patients (headache, nausea, and neurological changes from rapid fluid and osmolality shifts), and assessing the access site for bleeding or hematoma. For peritoneal dialysis, the most serious complication is peritonitis — presenting as cloudy effluent, abdominal pain, fever, and nausea — which requires immediate notification and antibiotic treatment instilled directly into the peritoneal cavity.
Endocrine Nursing: Diabetic Emergencies and Thyroid Crises
Endocrine nursing in NCLEX medical surgical nursing is dominated by diabetic emergencies and thyroid disorder complications — conditions where delayed recognition and intervention produce rapidly escalating patient harm.
DKA vs. HHS: The Critical Distinction
Diabetic ketoacidosis and hyperosmolar hyperglycemic state are the two diabetic hyperglycemic emergencies consistently tested in NCLEX medical surgical nursing. DKA occurs primarily in type 1 diabetes, is characterized by absolute insulin deficiency leading to ketone production and metabolic acidosis, and presents with blood glucose typically 250 to 600 mg/dL, deep rapid Kussmaul respirations compensating for metabolic acidosis, fruity acetone breath, nausea and vomiting, dehydration, and a positive serum ketone level. HHS occurs primarily in type 2 diabetes, involves relative insulin deficiency without significant ketone production, and presents with extreme hyperglycemia typically above 600 mg/dL and often above 1,000 mg/dL, profound dehydration and hyperosmolality, neurological symptoms including altered consciousness and seizures, but without the Kussmaul respirations or fruity breath of DKA because ketoacidosis is absent. Both require IV fluid replacement with isotonic saline as the first intervention, followed by insulin infusion and electrolyte replacement. The NCLEX medical surgical nursing potassium rule for both conditions: replace potassium before or concurrently with insulin administration if serum potassium is below 3.5 mEq/L — insulin drives potassium into cells and can precipitate fatal hypokalemia if the electrolyte deficit is not corrected first.
Hypoglycemia: The Rule of 15
Hypoglycemia management is one of the most frequently tested endocrine concepts in NCLEX medical surgical nursing because it requires both immediate intervention and accurate knowledge of the specific treatment sequence. Blood glucose below 70 mg/dL in a conscious patient is treated with the rule of 15: administer 15 grams of fast-acting carbohydrate — 4 ounces of juice, 3 to 4 glucose tablets, or 8 ounces of regular milk — wait 15 minutes, and recheck blood glucose. If still below 70 mg/dL, repeat the 15-gram carbohydrate and wait another 15 minutes. Once blood glucose is above 70 mg/dL, provide a snack containing protein and complex carbohydrate to prevent recurrence. For unconscious patients or patients unable to swallow, IV dextrose 50 percent is administered, or glucagon IM or subcutaneously if IV access is unavailable. The NCLEX medical surgical nursing safety rule: never give oral glucose to an unconscious patient because of aspiration risk.
Thyroid Crisis and Myxedema Coma
Thyroid storm — thyrotoxic crisis — is a life-threatening exacerbation of hyperthyroidism typically precipitated by infection, surgery, or trauma in a patient with uncontrolled or undiagnosed hyperthyroidism. The NCLEX medical surgical nursing presentation includes extreme hyperthermia, severe tachycardia and hypertension, diaphoresis, agitation, and altered consciousness. Immediate nursing priorities include cooling measures for hyperthermia, cardiac monitoring, IV fluid replacement, and administering ordered antithyroid medications, beta-blockers for cardiovascular stabilization, and corticosteroids. Myxedema coma is the life-threatening extreme of hypothyroidism and presents as the clinical opposite: hypothermia, bradycardia, hypotension, hypoventilation, and significantly altered consciousness. Both conditions are medical emergencies requiring ICU-level care and immediate provider notification.
Gastrointestinal Nursing: Priority Assessment and Post-Operative Care
Gastrointestinal nursing in NCLEX medical surgical nursing tests bowel assessment principles, GI bleed recognition and management, post-operative GI care, and inflammatory bowel conditions.
GI Bleed: Upper vs. Lower
Gastrointestinal bleeding questions in NCLEX medical surgical nursing test the ability to distinguish upper from lower GI bleeding by presentation and apply the correct priority assessment and interventions. Upper GI bleeding — from the esophagus, stomach, or duodenum — presents as hematemesis (vomiting blood, bright red or coffee-ground appearance) and melena (black, tarry, malodorous stool from digested blood). Lower GI bleeding — from the colon or rectum — presents as hematochezia (bright red blood from the rectum), which can also occur with massive upper GI bleeding due to rapid transit. The NCLEX medical surgical nursing priority for any active GI bleed is hemodynamic assessment: tachycardia is the earliest sign of significant blood loss, followed by hypotension as intravascular volume depletion progresses. Establishing large-bore IV access, preparing for fluid resuscitation and blood transfusion, placing the patient on NPO status, and notifying the provider are concurrent priorities in the acute management phase.
Bowel Obstruction: Small vs. Large
Bowel obstruction questions in NCLEX medical surgical nursing test assessment distinctions between small and large bowel obstruction and the priority interventions for each. Small bowel obstruction presents with high-pitched hyperactive bowel sounds early (borborygmi) progressing to absent sounds as the bowel dilates and motility ceases, early and frequent vomiting that may be bilious, and colicky cramping periumbilical pain. Large bowel obstruction presents with distension as the dominant finding, minimal or late vomiting, obstipation (inability to pass stool or flatus), and lower abdominal pain. The most dangerous complication of bowel obstruction is strangulation — compromised blood supply to the bowel wall — which presents with signs of peritonitis: rigid abdomen, rebound tenderness, fever, and signs of septic shock. The NCLEX medical surgical nursing nursing priorities for bowel obstruction include NPO status, nasogastric tube decompression, IV fluid resuscitation, and monitoring for strangulation signs requiring emergency surgical intervention.
Post-Operative GI Care and NG Tube Management
Post-operative GI nursing is a high-yield NCLEX medical surgical nursing topic because it integrates multiple assessment skills and safety principles. Assessment for return of bowel function after abdominal surgery includes auscultating bowel sounds in all four quadrants — return of bowel sounds indicates restoration of peristalsis and precedes safe resumption of oral intake — monitoring for flatus, and assessing the abdomen for distension and tenderness. For patients with nasogastric tubes: maintain tube patency by irrigating with normal saline as ordered, keep the tube on low continuous or intermittent suction as prescribed, assess gastric aspirate color and quantity, and monitor electrolytes for hyponatremia and hypokalemia from prolonged nasogastric drainage. Postoperative ileus — absence of bowel motility after surgery — is detected by absent bowel sounds, abdominal distension, nausea and vomiting, and inability to pass flatus. Early ambulation is the most effective NCLEX medical surgical nursing nursing intervention for preventing and resolving postoperative ileus.
- Crohn’s disease vs. ulcerative colitis key distinction: Crohn’s disease involves transmural inflammation affecting any part of the GI tract from mouth to anus, with skip lesions and the risk of fistula and abscess formation. Ulcerative colitis involves mucosal inflammation limited to the colon, progressing continuously from the rectum proximally. The highest-yield NCLEX medical surgical nursing distinction is that UC carries significantly higher colorectal cancer risk with long-standing disease, while Crohn’s carries higher risk of intestinal obstruction from strictures and fistula formation.
- Liver failure priority assessment: Hepatic encephalopathy — altered mental status from ammonia accumulation in liver failure — is assessed using neurological status monitoring and asterixis (flapping tremor of the extended wrist). Lactulose is the priority medication, reducing ammonia absorption from the colon. Bleeding risk from coagulopathy requires fall precautions, avoiding IM injections, and monitoring for spontaneous bleeding.
Cross-Cutting NCLEX Medical Surgical Nursing Principles
Beyond individual body system content, several clinical reasoning principles apply across all NCLEX medical surgical nursing scenarios and appear repeatedly at the highest difficulty levels of the exam.
Post-Operative Assessment: The Universal Priority Sequence
Post-operative assessment questions are among the most common NCLEX medical surgical nursing question types because they integrate multiple body systems, require nursing process sequencing, and test the ability to identify which post-operative finding is the highest priority. The universal post-operative assessment sequence follows the ABCs: airway patency and respiratory rate first — respiratory depression from anesthesia and opioid analgesics is the most common immediately life-threatening post-operative complication; then cardiovascular status — heart rate and blood pressure establishing hemodynamic stability; then surgical site assessment — dressing integrity, drainage characteristics, and evidence of hemorrhage; then neurological status — level of consciousness and return from anesthesia; then pain assessment. This sequence determines the priority answer in any post-operative scenario where multiple assessment findings are present.
Recognizing Sepsis and Septic Shock
Sepsis recognition is a high-yield cross-cutting NCLEX medical surgical nursing topic because it appears in scenarios from every body system — urinary tract infection progressing to urosepsis, pneumonia progressing to sepsis, surgical site infection, line-associated infection. The NCLEX medical surgical nursing sepsis recognition findings include fever above 38.5 degrees Celsius or hypothermia below 36 degrees, tachycardia above 90 bpm, tachypnea above 20 breaths per minute, altered mental status, and signs of organ dysfunction — elevated creatinine, lactate above 2 mmol/L, decreased urine output, or worsening oxygenation. Septic shock adds refractory hypotension despite adequate fluid resuscitation. The priority nursing interventions follow the sepsis bundle: obtain blood cultures before antibiotics, administer broad-spectrum antibiotics within one hour of recognition, begin IV fluid resuscitation, and measure serum lactate.
Pain Assessment and Opioid Safety
Pain management and opioid safety is a consistently tested NCLEX medical surgical nursing topic that integrates assessment, intervention, and evaluation skills. The numeric pain scale (0 to 10) is the most widely used validated tool for conscious adults — 0 is no pain, 10 is the worst imaginable pain. Before administering opioid analgesics, the NCLEX medical surgical nursing safety assessment includes respiratory rate — hold and notify the provider if below 12 breaths per minute — level of consciousness, and blood pressure. After opioid administration, reassess pain at the appropriate interval based on the route given: IV opioids are reassessed within 15 to 30 minutes; oral opioids within 60 minutes. Naloxone is the opioid reversal agent — kept available for all patients receiving IV opioids — and is administered for respiratory depression or unresponsiveness. The most important NCLEX medical surgical nursing safety principle for opioids: assess before administering, reassess after, and never administer to a patient with a respiratory rate below 12.
Conclusion
NCLEX medical surgical nursing is the content foundation that the exam is built on — and mastering it requires more than broad familiarity with each body system. It requires precise knowledge of which clinical findings signal the highest priority, which nursing interventions are indicated at which point in the nursing process, and which cross-cutting principles apply consistently across scenarios regardless of the specific system involved. The cardiovascular, respiratory, neurological, renal, endocrine, and gastrointestinal content covered in this guide represents the most consistently tested NCLEX medical surgical nursing topics — the ones that appear at every difficulty level and across both traditional and NGN question formats.
Study NCLEX medical surgical nursing through active recall rather than passive review — close your notes and generate the clinical distinction between DKA and HHS, the priority nursing actions for tension pneumothorax versus simple pneumothorax, the position rule for arterial versus venous insufficiency, and the emergency sequence for autonomic dysreflexia. The clinical reasoning the exam tests in this content area is not memorization of facts — it is the ability to apply those facts correctly in a complex patient scenario where multiple findings compete for priority attention. Build that reasoning through deliberate practice, and the most heavily weighted section of the exam becomes your strongest performance area.