NGN case study questions are the most clinically sophisticated assessment format the NCLEX has ever used — and the most challenging for candidates whose preparation has been built primarily on traditional multiple choice practice. The Next Generation NCLEX launched in April 2023 with five distinct format types designed to measure clinical judgment in ways that single-best-answer questions cannot: unfolding case study sets, bow tie questions, extended multiple response, matrix multiple choice, and trend questions. Among these, NGN case study questions — specifically the unfolding case study sets — represent the highest cognitive complexity because they require sustained clinical reasoning across a six-question set that progressively reveals a patient’s clinical situation, demanding that each question be answered not in isolation but within the context of a developing clinical narrative.
The candidates who struggle most with NGN case study questions are frequently those who are strongest at traditional NCLEX multiple choice — because the cognitive skills that produce high accuracy on single-best-answer questions are partly different from those that produce high accuracy on unfolding case study sets. The traditional NCLEX rewards pattern recognition: the ability to identify a clinical scenario as matching a known clinical situation and select the option that corresponds to the correct management of that situation. NGN case study questions reward clinical reasoning process: the ability to recognize individual cues within an evolving patient narrative, analyze their combined significance, prioritize the clinical hypotheses they support by urgency, generate appropriate solutions, select the correct action for the current clinical moment, and evaluate whether prior actions achieved their intended outcomes — six sequential cognitive processes that must be applied in the correct sequence to the same patient across six consecutive questions. This guide provides the complete strategy for each of these cognitive processes and each of the five NGN format types, building the clinical judgment architecture that NGN case study questions measure.
This guide covers the complete NGN strategy for 2026: the CJMM cognitive skill framework that governs every NGN question type, the specific strategy for each of the five NGN format types with worked examples, the unfolding case study integration approach that prevents the most common NGN case study question error, the partial credit mechanics that distinguish NGN scoring from traditional scoring, the preparation approach that builds NGN clinical judgment as an automatic reasoning reflex rather than a deliberately applied technique, and the preparation schedule integration that ensures NGN performance matches traditional format performance by exam day.
The CJMM Framework: The Architecture Behind Every NGN Question
Every NGN case study question, bow tie, extended multiple response, matrix, and trend question is designed to measure one or more of the six Clinical Judgment Measurement Model cognitive skills. Understanding which skill each question type measures is the foundational NGN strategy — because it determines what cognitive process the question is testing and therefore what the correct answer should demonstrate.
The Six Cognitive Skills and Their Question Mapping
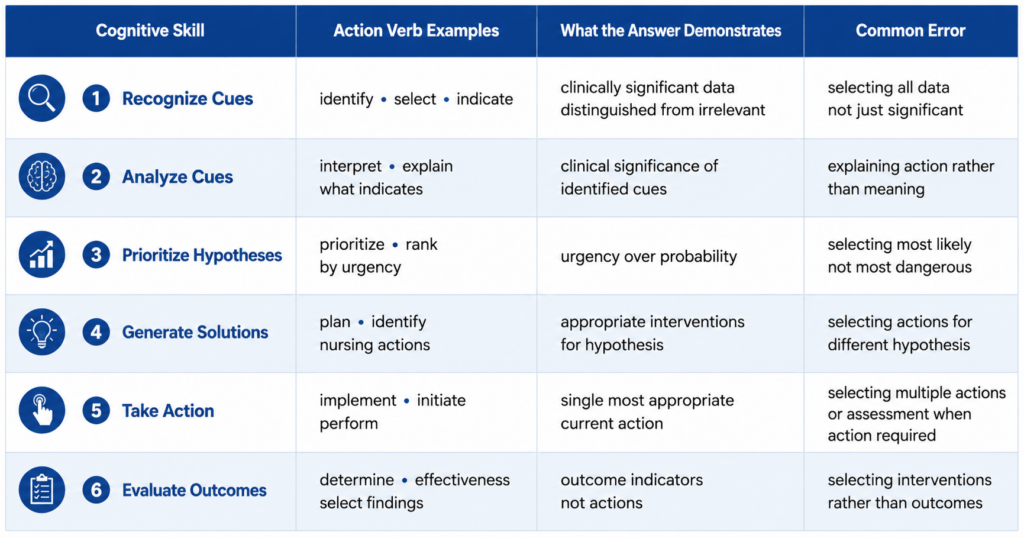
The six CJMM cognitive skills map onto NGN question types in specific, consistent ways that allow a trained candidate to identify the cognitive skill being tested from the question’s action verb before engaging any answer options. Recognize cues questions use action verbs like identify, select, or indicate and ask the candidate to identify which clinical data from a scenario are the most relevant, significant, or abnormal. The answer demonstrates the ability to distinguish clinically significant from clinically irrelevant data — not every piece of patient information in a scenario is a cue requiring action, and the recognize cues question tests whether the candidate can identify which data warrant clinical attention. Analyze cues questions use action verbs like interpret, explain, or determine what the data indicates and ask the candidate to explain the clinical significance of already-identified cues. The answer demonstrates understanding of what the clinical data means about the patient’s condition — connecting the cue to its clinical implication. Prioritize hypotheses questions present multiple possible clinical explanations and ask which is the highest priority or most urgent concern — the urgency-over-probability principle governs: the hypothesis that would cause the most immediate harm if correct takes priority regardless of statistical likelihood. Generate solutions questions ask what nursing actions or interventions are indicated for the identified hypothesis. Take action questions ask what the nurse does first or immediately — the single most appropriate nursing action for the current clinical moment given the established priority. Evaluate outcomes questions ask what findings indicate the nursing action was effective — shifting from action selection to outcome identification.
Action Verb Identification as the Pre-Option Strategy
The single most important NGN strategy applicable across all NGN case study questions and other NGN format types is action verb identification — reading the question stem’s action verb before engaging any answer option and using it to name the CJMM cognitive skill being tested. An action verb of identify or select indicates a recognize cues or generate solutions question. An action verb of interpret or indicate what this finding suggests indicates an analyze cues question. An action verb of prioritize or rank by urgency indicates a prioritize hypotheses question. An action verb of implement or perform or initiate indicates a take action question. An action verb of determine whether the intervention was effective or select findings that indicate improvement indicates an evaluate outcomes question. This action verb identification takes three to five seconds per question and directly names the cognitive framework that the correct answer must demonstrate — which eliminates the most common NGN case study question error of applying the wrong cognitive skill to a question (selecting an intervention option in a recognize cues question, or selecting a data point when the question requires an action).
The CJMM Applied to Unfolding Case Study Sets
In NGN case study questions organized as unfolding case study sets, the six CJMM cognitive skills typically appear in a sequence that mirrors the clinical judgment process — recognize cues first, then analyze cues, then prioritize hypotheses, then generate solutions or take action, then evaluate outcomes — though not every set includes all six skills and the ordering may vary. The strategic implication is that each question in the set builds on the clinical judgment established by the previous questions. The patient who was identified as showing early signs of septic shock in question one of the set — recognized cues including fever, elevated heart rate, low blood pressure, and decreased urine output — carries that developing clinical picture into question two’s analyze cues question, question three’s prioritize hypotheses question, and the subsequent take action and evaluate outcomes questions. Treating each question in the set as a standalone scenario — rather than as the next step in a continuous clinical reasoning process — is the most common and most preparation-addressable NGN case study question error.
The Five NGN Format Types: Strategies for Each

Beyond the CJMM cognitive skill framework that governs what each question tests, the five NGN format types each have specific mechanics, scoring rules, and response strategies that require format-specific preparation.
Unfolding Case Study Sets: The Integration Strategy
Unfolding case study sets are the flagship NGN format — six questions anchored to a single patient scenario that progressively reveals clinical information across the question sequence. The integration strategy for NGN case study questions in unfolding sets has three components. First, read the opening scenario as a complete clinical picture document rather than as the stem of the first question — extract the patient demographics, presenting situation, vital signs, history, and any assessment data provided and hold them as the developing clinical narrative that all six questions will reference. Second, carry forward the established clinical picture from each previous question into each subsequent question — the patient’s condition established in question one continues to develop in questions two through six, and each question assumes the candidate has retained the accumulating clinical data rather than starting fresh. Third, apply the correct CJMM cognitive skill for each question independently — the recognize cues skill applied in question one does not mean question two requires recognize cues; identify the action verb for each question individually rather than assuming the set follows a fixed CJMM sequence.
Bow Tie Questions: The Center-First Strategy
The bow tie question presents a structured diagram with a center condition identification, left-side actions, and right-side monitoring parameters. The format name reflects its visual shape — two triangles connected at the center point. The bow tie strategy for NGN case study questions and standalone bow tie items has a specific sequence: identify the center condition first. The center condition is the priority clinical problem or hypothesis that the patient’s scenario data supports — and the correct center condition selection determines which actions and monitoring parameters are correct, because actions and monitoring parameters that are appropriate for one condition may be incorrect or harmful for another. Select the center condition using the prioritize hypotheses principle (most urgent over most likely), then work outward from the confirmed center to select the matching actions (nursing interventions appropriate for the center condition) and monitoring parameters (assessment findings that would confirm the condition is progressing or responding). Bow tie questions are scored with partial credit — center condition alone does not earn full credit, and correct actions and monitoring without the correct center earns partial credit only.
Extended Multiple Response: The Independent Criteria Strategy
Extended multiple response questions present five to eight options and ask the candidate to select all that apply — with no indication of how many correct options exist. The independent criteria strategy is the most important tactical approach for NGN case study questions in this format: evaluate each option independently against the clinical criteria established by the scenario rather than comparatively against other options. Ask of each option individually: given this patient’s specific situation, does this option meet the clinical criteria for being indicated, safe, appropriate, and prioritized for this patient at this clinical moment? If yes, select it. If no, do not. This independent evaluation prevents the two most common extended multiple response errors: selecting an option because it seems plausible relative to other options (comparative reasoning) and failing to select an option because another more obvious option already seems correct (satiation error). The partial credit scoring system rewards independent selection accuracy — selecting four of five correct options earns more credit than selecting three of five, making exhaustive independent evaluation of every option more valuable than selecting only the obvious ones.
Matrix Questions: The Row-by-Row Strategy
Matrix questions present a table with conditions or patients in rows and assessment findings or nursing actions in columns, asking the candidate to make a binary selection (indicated/not indicated, or effective/not effective) for each cell. The matrix strategy for NGN case study questions and standalone matrix items applies the row-by-row approach: complete all selections for one row before moving to the next, using the clinical context of that specific row (the specific condition or patient) as the reference frame for each column selection. Shifting attention between rows mid-matrix — selecting some cells in row one, then some in row two, then returning to row one — produces context contamination where the clinical frame of one row bleeds into the selection criteria of another. The partial credit mechanics in matrix questions are cell-by-cell — each correct cell selection earns partial credit, making thorough independent cell evaluation the optimal strategy rather than rushing to complete the matrix within a compressed time budget.
Trend Questions: The Baseline Comparison Strategy
Trend questions present clinical data across multiple time points — vital signs, laboratory values, or assessment findings recorded at two, three, or four intervals — and ask the candidate to interpret the trend’s clinical significance or identify the appropriate nursing response to the demonstrated trend. The baseline comparison strategy for NGN case study questions in trend format is evaluating each time-point value not against absolute normal ranges but against the patient’s established baseline and the direction of change — because a value that is abnormal by population standards but stable from the patient’s documented baseline carries different clinical significance than the same value that represents a new deterioration from a normal baseline. The action verb in trend questions typically asks the candidate to analyze what the trend indicates (analyze cues skill) or to select the most appropriate nursing response to the trend direction (take action skill). A worsening trend in a deteriorating clinical parameter requires identification of the clinical implication and the appropriate escalation action even when each individual value would not independently trigger concern.
The Partial Credit System: How NGN Scoring Works
The partial credit scoring system for NGN case study questions and other NGN format types is fundamentally different from traditional NCLEX scoring and requires a specific response strategy that maximizes partial credit rather than optimizing for single-best-answer selection.
How Partial Credit Is Calculated
NGN partial credit scoring awards points for each correct response element and deducts points for each incorrect response element, within a defined maximum score for each question. The exact deduction structure varies by question type and item, but the consistent principle across all NGN case study questions and other partial credit formats is that selecting incorrect elements reduces the partial credit earned — not just failing to earn additional credit. This means the optimal partial credit strategy is not selecting every option that might be correct but applying clinical criteria rigorously to exclude options that fail the criteria before selecting. A candidate who selects all five correct options and also selects two incorrect options earns less credit than a candidate who selects four of five correct options and no incorrect options — because the two incorrect selections produce deductions that offset the credit earned from the fifth correct option. The strategy implication is conservative confidence: select an option only when the clinical criteria clearly support its inclusion, not when it seems possibly relevant or vaguely related to the clinical scenario.
The Conservative Confidence Threshold
The conservative confidence threshold for NGN case study questions is the decision rule that applies the partial credit mechanics to the response selection process: select an option when clinical reasoning clearly establishes that it meets the criteria the question specifies — not when it might meet the criteria or when it is difficult to definitively exclude. This threshold is lower than the threshold that would maximize the selection of correct options in isolation (which would favor generous inclusion) and higher than the threshold that would avoid all uncertainty (which would produce under-selection of correct options). In practice, the conservative confidence threshold means: for each option in an extended multiple response or matrix question, apply the four-question clinical verification: is this option clearly indicated for this specific patient at this specific clinical moment, would a well-prepared nurse identify this option as required without hesitation, does excluding this option represent a clinical error rather than a conservative judgment, and does the scenario data specifically support this option rather than merely not contradict it? If yes to all four, select confidently. If uncertain about any, apply clinical criteria more carefully before selecting.
Tracking Your NGN Accuracy Separately
The partial credit mechanics of NGN case study questions mean that overall accuracy tracking — which combines traditional and NGN format performance into a single percentage — obscures the NGN-specific performance gap that most candidates have. A candidate with 63 percent overall accuracy composed of 70 percent traditional format accuracy and 44 percent NGN format accuracy is not as prepared for the current examination as their overall number suggests, because the higher NGN format proportion of the April 2026 examination means the 44 percent NGN performance contributes to a larger share of the ability estimate than it did in 2023. Track NGN accuracy in a separate column in the weekly micro-audit, calculated from NGN-only question performance rather than from the aggregate. The NGN accuracy benchmark of 50 percent or above is the target — and it must be tracked independently to be managed rather than absorbed into an overall number that conceals the format gap.
The Unfolding Case Study Integration Technique
The unfolding case study integration technique is the specific preparation skill that prevents the most common and most preparation-addressable error in NGN case study questions — treating each question in the set as a standalone scenario rather than as the next step in a continuous clinical reasoning process.
Building the Clinical Narrative Before Question One
The integration technique begins before answering any question in the NGN case study set — with a deliberate reading of the opening scenario as a complete clinical narrative rather than as question-one context only. Read the scenario and extract: the patient’s age, relevant history, the presenting situation, all vital signs and laboratory values provided, any assessment findings described, and the clinical setting. Build a brief mental or written clinical picture: this is a 67-year-old post-surgical patient, three days post-laparotomy, presenting with fever, elevated heart rate, hypotension, decreased urine output, and elevated WBC. This clinical picture is not the answer to question one — it is the patient narrative that all six questions will reference. Establishing it deliberately before engaging question one prevents the most common early-set error: answering the first question without adequate clinical context, which produces an incomplete recognize cues selection that compromises the clinical narrative available for all subsequent questions in the set.
The Carry-Forward Protocol Between Questions
Between each question in an NGN case study set, the carry-forward protocol applies before engaging the next question’s stem: review what the previous question established about the patient’s clinical situation. Question one established that the patient has fever, tachycardia, hypotension, and elevated WBC — possible early sepsis. Question two added that lactate is 2.8 mmol/L, oxygen saturation is 94 percent on room air, and the patient is increasingly confused — the clinical picture is now consistent with septic shock. Question three asks to prioritize hypotheses: the carry-forward protocol ensures that the question three analysis incorporates the full clinical picture accumulated across questions one and two rather than only the data presented in question three’s stem. This protocol is the mechanical implementation of the unfolding case study’s core clinical reasoning demand — sustained narrative integration rather than question-by-question pattern matching.
Managing Time Across a Six-Question Set
NGN case study questions in unfolding sets are time-intensive relative to traditional questions — the extended reading required for the scenario plus six questions, the partial credit evaluation required for each option, and the carry-forward integration required between questions collectively require more than the 90-second average that traditional questions use. The practical time management strategy for unfolding case study sets is allocating eight to ten minutes for the complete six-question set rather than applying the 90-second per question standard individually. Within the set, recognize cues and analyze cues questions typically take less time (identifying relevant data is faster than applying multiple criteria for each option), while extended multiple response and matrix questions within the set take more time (independent criteria evaluation per option is thorough). The overall eight-to-ten minute budget for a complete NGN case study set produces a total session time impact equivalent to approximately six traditional questions — which means the pacing impact of unfolding case study sets on total session timing is less disruptive than candidates often fear, provided the set is approached as a unified time block rather than question-by-question with individual time budgets.
Building NGN Fluency: The Preparation Approach
NGN case study question fluency — the ability to navigate NGN formats with the automatic clinical reasoning that produces consistently high partial credit scores — is built through specific preparation practices that standard question bank practice does not automatically develop.
The CJMM Skill Identification Practice
The foundational NGN preparation practice is the CJMM skill identification drill — applied to every NGN question in every practice session before any option is engaged. Before reading answer options in any NGN case study question or other NGN format item, identify the CJMM cognitive skill from the action verb: this is a recognize cues question, this is a take action question, this is an evaluate outcomes question. Record the identification. After the question is answered and the rationale is reviewed, compare the identified skill against what the rationale confirms the question was testing. Mismatches between the pre-option identification and the rationale’s skill label reveal the specific action verbs or question structures that are being misread as different cognitive skills — which is the most precise preparation intelligence available for targeting NGN accuracy improvement. The CJMM skill identification drill builds the automatic action verb recognition that allows NGN case study questions to be approached from the correct cognitive framework before distractors create competing clinical associations.
The Full Set Practice Requirement
NGN case study questions in unfolding sets must be practiced as complete sets rather than as individual questions extracted from their narrative context. Many question bank platforms allow filtering by question type — and some candidates practice NGN content by selecting individual extended multiple response or matrix questions without completing full unfolding case study sets. This practice builds partial-credit response mechanics without building narrative integration — which is the specific skill that the unfolding case study format most heavily tests and that most distinguishes high and low NGN performance among candidates with similar traditional format accuracy. At least two complete unfolding case study sets should be practiced per week from the beginning of NGN-specific preparation — full six-question sets read as integrated clinical narratives with the carry-forward protocol applied between questions. The NCSBN official NGN sample questions at ncsbn.org provide the most authoritative format reference and should be completed as full sets at the beginning of NGN preparation to establish format expectations before beginning question bank NGN sessions.
The NGN Rationale Review Protocol
The rationale review protocol for NGN case study questions differs from the standard four-question protocol used for traditional questions in one important addition: after reviewing the clinical content of the correct answer and the reasons each incorrect option fails, identify which specific CJMM cognitive skill the question was testing and whether the approach applied to the question matched that skill. A candidate who answered a prioritize hypotheses question by selecting the most commonly occurring clinical explanation rather than the most urgently dangerous one has committed a specific CJMM skill error — applying probability reasoning to a question that required urgency reasoning — and the rationale review should explicitly name this as a CJMM skill application error rather than as a content error. This distinction determines the preparation response: a content error requires content review; a CJMM skill application error requires deliberate practice of the urgency-over-probability principle applied to prioritize hypotheses questions specifically. The NGN rationale review protocol that names the CJMM skill and the error type produces preparation intelligence that the standard rationale protocol does not.
- Weekly NGN practice minimum for exam readiness: A minimum of 25 percent of weekly practice questions should be NGN format items, increasing to 30 to 35 percent as the exam date approaches. At least two complete unfolding case study sets per week should be completed as integrated full-set practices rather than as individual extracted questions. The CJMM skill identification drill should be applied to every NGN question — not only to incorrect answers — to build both correct skill identification for questions answered correctly and identification of the skill misapplication that produced incorrect answers.
- The NGN benchmark and how to track it: Track NGN accuracy in a separate weekly record from overall accuracy. NGN accuracy at 50 percent or above is the benchmark — and achieving it requires separate tracking to manage it. A useful tracking format records the total NGN questions completed in the week, the number of NGN partial credit points earned versus possible, and the specific NGN format types where accuracy is lowest. The format-specific breakdown (unfolding case study sets below standard while bow tie questions are above standard, for example) identifies the most targeted preparation intervention rather than treating NGN as a single undifferentiated category.
- Using the NCSBN official NGN samples as the preparation anchor: The NCSBN official NGN sample questions available at ncsbn.org are the only authoritative format reference for current NCLEX NGN specifications. Complete them at the beginning of NGN preparation to calibrate format expectations, again at the midpoint of preparation to assess whether format fluency has developed, and again in the final week as a format calibration check before the exam. Third-party question banks vary in their NGN format accuracy and CJMM skill alignment — using the official samples as the anchor prevents calibrating preparation against a format approximation that differs from the actual examination.
Conclusion
NGN case study questions are the most clinically rigorous assessment format on the current NCLEX — and the most rewarding to prepare for when the preparation is organized around the CJMM cognitive skill framework rather than around format mechanics alone. The six cognitive skills govern what every NGN question tests; action verb identification reveals which skill applies before options create competing clinical associations; the five format-specific strategies optimize partial credit across the five distinct question types; the unfolding case study integration technique prevents the most common and most damaging NGN error; and the partial credit conservative confidence threshold balances thorough option evaluation against the deduction risk of including incorrect options.
The candidates who perform best on NGN case study questions are not those who have practiced the most NGN questions — they are those who have practiced with CJMM skill identification applied to every question, carry-forward integration applied to every unfolding set, independent criteria evaluation applied to every option in every partial credit format, and specific NGN accuracy tracked separately from overall accuracy so that the format gap can be identified and closed before the exam. Build these practices from the first week of NGN-specific preparation. Apply them consistently through the full preparation period. Arrive at the exam knowing that the clinical judgment the NGN case study questions test has been developed as an automatic reasoning reflex — not a consciously retrieved technique but the natural expression of weeks of deliberate clinical reasoning practice at the NGN format’s highest cognitive demands.