NCLEX question types in 2026 are more varied and more cognitively demanding than at any previous point in the exam’s history. The Next Generation NCLEX launched in 2023 introduced five new question formats built around the NCSBN Clinical Judgment Measurement Model — formats that test clinical reasoning at a structural level that traditional multiple choice cannot reach. A candidate who walks into the testing center without a clear, working understanding of every NCLEX question type they will encounter is at a genuine disadvantage that no amount of content knowledge or practice question volume fully compensates for.
Format familiarity matters for two distinct reasons. The first is cognitive efficiency: a candidate who encounters an unfolding case study for the first time on exam day must simultaneously decode the format structure and apply clinical reasoning to it. That dual cognitive load is avoidable through preparation. A candidate who has practiced every NCLEX question type extensively before exam day processes the format automatically and directs full cognitive capacity to the clinical judgment the question is testing. The second reason is scoring mechanics: the NGN question types use scoring models that differ from traditional binary correct-or-incorrect scoring. Understanding how partial credit works for extended multiple response items and how the CJMM cognitive skills map to unfolding case study questions changes how candidates engage with these items in ways that directly affect the score they contribute to the ability estimate.
This guide covers every NCLEX question type candidates will encounter on the 2026 exam: the traditional formats that have been part of the exam for decades and remain a significant portion of the item pool, and the five Next Generation NCLEX formats introduced to assess clinical judgment across the full CJMM cognitive skill sequence. For each question type, the guide explains the structural format, what cognitive skill it is testing, how it is scored, and the specific preparation and engagement strategy that produces the strongest performance on that format.
How NCLEX Question Types Are Organized in 2026
Before examining individual formats, understanding how NCLEX question types are organized within the broader exam structure clarifies why each format exists and what it is specifically designed to measure.
Two Categories: Standalone and Case-Based
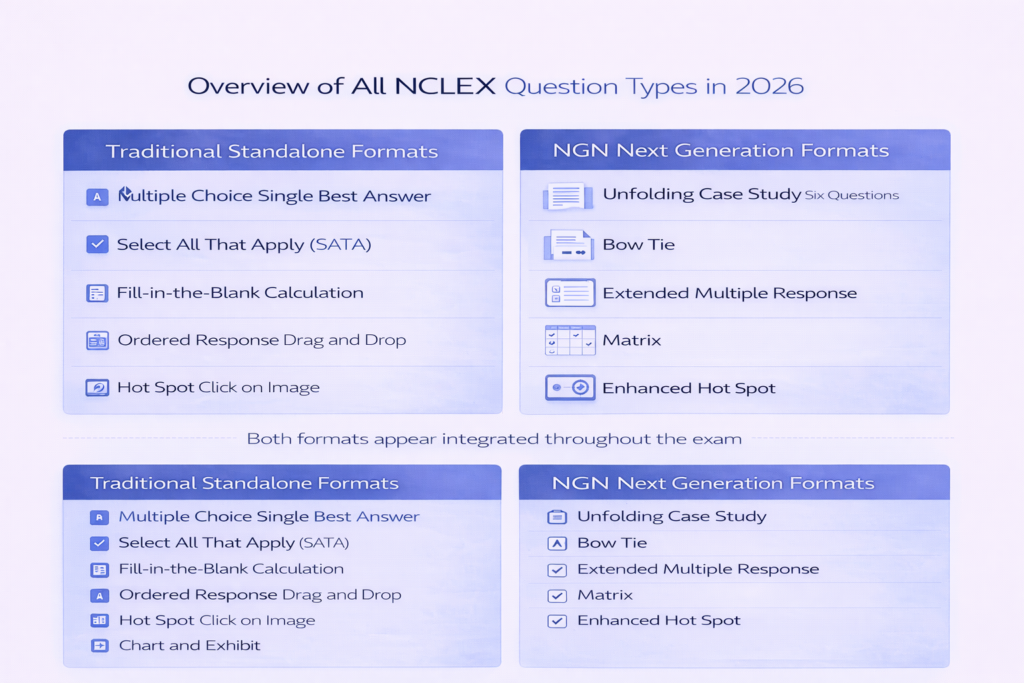
All NCLEX question types in 2026 fall into one of two structural categories: standalone items and case-based items. Standalone items present a self-contained clinical scenario that provides all information needed to answer the question within a single item. Traditional multiple choice, select all that apply, fill-in-the-blank calculation, ordered response, hot spot, and chart and exhibit questions are all standalone NCLEX question types — each complete in itself with no dependency on preceding or following items. Case-based items present a clinical scenario that unfolds across multiple related questions, with each question building on or extending the clinical situation established in the scenario introduction. The unfolding case study is the primary case-based NCLEX question type in 2026, presenting six questions that follow a single patient through a clinical encounter.
The Clinical Judgment Measurement Model Framework
The Next Generation NCLEX question types are organized around the NCSBN Clinical Judgment Measurement Model, which defines six cognitive skills that competent entry-level nurses must apply in clinical practice: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, and evaluate outcomes. Each of the five NGN NCLEX question types is designed to test one or more of these cognitive skills at a level of structural complexity that traditional multiple choice cannot replicate. Unfolding case studies test all six skills sequentially across the six-question set. Bow tie questions test analyze cues, prioritize hypotheses, and take action simultaneously within a single integrated item. Extended multiple response, matrix, and enhanced hot spot items test specific cognitive skills in a polytomous format that awards partial credit based on the number of correct selections. Understanding this framework makes every NGN NCLEX question type conceptually coherent rather than a collection of unfamiliar formats to memorize.
Traditional and NGN Formats Both Appear Throughout
A common misconception about NCLEX question types in 2026 is that the exam is divided into a traditional section and an NGN section. It is not. Both traditional and NGN formats appear distributed throughout the exam session without a defined boundary between them. A candidate may receive a traditional multiple choice question followed by an unfolding case study followed by more traditional questions followed by a bow tie. The NGN NCLEX question types are integrated into the full item pool rather than clustered together, which means candidates must be ready to shift between format modes throughout the exam rather than at a specific point in the session. This integration makes format familiarity with all NCLEX question types — not just the traditional ones — essential for consistent exam performance.
Traditional NCLEX Question Types: Formats That Remain Central

Traditional NCLEX question types continue to form a significant portion of the item pool in 2026. Mastery of these formats remains essential — not only because they appear frequently but because the clinical reasoning habits they require are the foundation on which NGN format engagement is built.
Multiple Choice: Single Best Answer
Single best answer multiple choice is the most familiar of all NCLEX question types and the format most candidates have the most practice with from nursing school exams. A clinical scenario stem is followed by four answer options, and the candidate selects the single most correct response. The cognitive demand is not identifying a correct answer but selecting the best answer — the option that most directly addresses the highest clinical priority, at the correct nursing process step, for the specific patient in the scenario. The most common error on this NCLEX question type is not a knowledge error but a reasoning error: selecting an option that is clinically reasonable in general rather than clinically optimal for the specific scenario. The two-read discipline — first read for clinical situational awareness, second read for action verb identification — and the clinical reasoning framework sequence (ABCs, Maslow, nursing process, safety) produce consistent performance on this format when applied systematically.
Select All That Apply (SATA)
Select all that apply is the traditional multiple response NCLEX question type and one of the most anxiety-producing formats for many candidates. A clinical scenario is followed by five or six answer options, and the candidate selects every option that applies — there is no defined number of correct answers, and traditional NCLEX scoring for this format is all-or-nothing: all correct options must be selected and no incorrect options included for full credit. The most effective engagement strategy for this NCLEX question type is independent evaluation of each option against the clinical scenario — asking of each option individually whether it is clinically applicable for this specific patient, yes or no, before moving to the next. Comparative evaluation — ranking which options seem most correct across the list — consistently produces both false negatives (missing correct options that seem less dramatic) and false positives (including incorrect options that seem plausible). The independent yes-or-no evaluation applied to each option in sequence is the specific habit that improves SATA accuracy.
Fill-in-the-Blank Calculation
Calculation questions are a standalone NCLEX question type that present a medication dosage, IV flow rate, or unit conversion problem requiring a numerical answer entered into a blank field. The on-screen calculator is available for all calculation NCLEX question types and should always be used — mental arithmetic under exam pressure introduces calculation errors that the calculator eliminates entirely. The most effective preparation strategy is a consistent dimensional analysis sequence applied to every calculation: identify what is given, identify what unit is asked for, set up the conversion chain or formula, calculate, and verify that the unit of the final answer matches what the question requested. A consistent calculation sequence is faster than an improvised one because the steps are automated rather than reconstructed from scratch for each problem.
Ordered Response
Ordered response questions present a set of nursing actions, assessment steps, or clinical interventions and ask the candidate to arrange them in the correct sequence by dragging and dropping items into a numbered order. This NCLEX question type most directly tests nursing process sequencing and clinical prioritization — the same reasoning that single best answer questions test through option selection, ordered response tests through arrangement. The most common error on this format is placing intervention steps before assessment steps in non-emergency scenarios, or sequencing safety actions after clinical care actions when immediate safety is the clinical priority. The same nursing process and priority framework logic that governs single best answer selection governs ordered response arrangement — assessment before intervention except in ABC emergencies, safety before comfort, physiological before psychosocial.
Hot Spot and Chart and Exhibit
Hot spot NCLEX question types present a clinical image — a body diagram, an ECG strip, a medication label, or an anatomical illustration — and ask the candidate to click on the specific area or finding that answers the question. Chart and exhibit questions present a multi-tab clinical record — vital sign flowsheets, laboratory result panels, medication administration records, provider orders — and ask the candidate to identify specific information or make a clinical judgment based on the data available across the tabs. Both formats test the ability to extract clinically relevant information from a complex visual display — a skill that parallels the real clinical task of identifying priority findings from a patient’s chart. The most common error on chart and exhibit NCLEX question types is not reviewing all available tabs before answering, which misses clinical data that changes the correct response.
NGN Question Types: The Five Next Generation NCLEX Formats
The five Next Generation NCLEX question types introduced in 2023 represent the most significant structural change to the exam in decades. Each format is designed to assess specific clinical judgment cognitive skills that traditional multiple choice cannot measure with sufficient granularity to confirm entry-level nursing competency.
1. Unfolding Case Study
The unfolding case study is the most complex and most time-intensive of all NCLEX question types. A single patient scenario — typically presenting a patient at a specific point in a clinical encounter — unfolds across six questions that follow the patient’s situation as it evolves. Each question maps to one of the six CJMM cognitive skills in sequence: question one tests recognize cues, question two tests analyze cues, question three tests prioritize hypotheses, question four tests generate solutions, question five tests take action, and question six tests evaluate outcomes. The scenario introduction provides the initial clinical data, and new information — updated vital signs, new laboratory results, the patient’s response to an intervention — is added before specific questions as the clinical situation evolves. Each question is scored independently using standard NCLEX scoring. The most critical preparation habit for this NCLEX question type is front-loaded scenario investment: read the scenario introduction thoroughly for question one, then read only the new clinical information added before subsequent questions rather than re-reading the entire scenario from the beginning for each item. Identifying the CJMM skill being tested from the action verb of each question — the nurse recognizes indicates recognize cues, the nurse analyzes indicates analyze cues — directs the correct type of clinical reasoning for each item within the set.
2. Bow Tie
The bow tie is the most visually distinctive of all NCLEX question types. It presents a clinical scenario and a three-section response structure: a center section where the candidate identifies the most likely condition or clinical problem, a left section where the candidate selects two priority nursing actions, and a right section where the candidate selects two parameters to monitor. The three sections form a bow tie shape around the central clinical judgment. Each selection within the bow tie may be scored independently or as a component of the integrated response, depending on platform implementation. The preparation and engagement strategy that produces the strongest bow tie performance is center-first commitment: identify the central condition most supported by the clinical data before selecting any actions or monitoring parameters. Attempting to complete all three sections simultaneously creates a circular reasoning loop where action selection and condition identification become confused. Once the central condition is identified and committed to, the actions and monitoring parameters that correctly follow from that specific condition are derivable from clinical knowledge of that condition rather than from general nursing knowledge applied globally. The bow tie NCLEX question type tests analyze cues (identifying the condition) and take action (selecting appropriate interventions and monitoring) simultaneously within a single integrated item.
3. Extended Multiple Response
Extended multiple response is the NGN evolution of the traditional SATA format and differs from it in two important ways: the option list may be longer (six or more options rather than five), and scoring is polytomous rather than all-or-nothing — partial credit is awarded based on the number of correct options selected relative to the total correct options available. This partial credit scoring mechanism is the most important scoring distinction across all NCLEX question types, and it directly changes the optimal engagement strategy. Because partial credit rewards every correct selection even when not all correct options are identified, thoughtful engagement with every option produces a stronger score contribution than rushing through the list or guessing. The independent yes-or-no evaluation strategy applies to this format as it does to traditional SATA, with the important addition that eliminating clearly incorrect options before committing to final selections is especially valuable when the list is long. Extended multiple response NCLEX question types test recognize cues and generate solutions cognitive skills, typically asking candidates to identify assessment findings that support a specific clinical hypothesis or to select appropriate interventions for a defined clinical situation.
4. Matrix
Matrix questions present a clinical scenario and a grid structure in which rows represent clinical variables or options and columns represent categories or conditions. The candidate makes a selection in each cell of the grid — for example, indicating whether each listed medication is appropriate to administer, or whether each assessment finding is expected or unexpected for a specific patient condition. Matrix NCLEX question types test clinical judgment across multiple dimensions simultaneously, requiring the candidate to apply consistent clinical reasoning to each row-column intersection rather than selecting a single correct answer from a list. Scoring may be polytomous — awarding partial credit for each correctly completed row or cell — or structured differently depending on the specific matrix format used. The most effective engagement strategy is row-by-row evaluation: complete all column selections for the first row before moving to the second row, proceeding sequentially rather than jumping between rows. This systematic approach prevents the disorientation of tracking multiple simultaneous dimensions and ensures every cell is evaluated. Matrix NCLEX question types most commonly test analyze cues and evaluate outcomes cognitive skills.
5. Enhanced Hot Spot
The enhanced hot spot is the NGN evolution of the traditional hot spot NCLEX question type, with the addition of text highlighting as an interaction mode alongside image clicking. Enhanced hot spot items present a clinical document — a nursing note, a provider order, a patient history, a medication administration record — and ask the candidate to highlight or click on the specific word, phrase, or finding that answers the question. The clinical document format mirrors the real nursing task of reading patient records and identifying priority information within a text-dense environment. Enhanced hot spot NCLEX question types most commonly test recognize cues — identifying the specific clinical finding in a document that signals a priority concern — and evaluate outcomes — identifying the specific documentation component that indicates a patient’s response to treatment. The most important preparation habit for this format is disciplined reading: read the full document before clicking rather than scanning for familiar terms, because the correct selection is sometimes a subtle finding that a scanning approach misses in favor of more prominent but clinically less significant terms.
How NGN Scoring Differs From Traditional NCLEX Question Scoring
Understanding how the NGN NCLEX question types are scored is essential for preparation because it changes the optimal engagement strategy for those formats and explains why partial engagement with NGN items is better than disengagement.
Dichotomous vs. Polytomous Scoring
Traditional NCLEX question types use dichotomous scoring: a response is either fully correct or incorrect. A single best answer question answered correctly earns the full item credit; answered incorrectly, it earns nothing. Traditional SATA is also scored dichotomously: all correct options must be selected and no incorrect options included for any credit, making partial selection worth nothing. Polytomous scoring — used for extended multiple response, matrix items, and some bow tie implementations — awards credit based on the degree of correctness rather than requiring complete accuracy for any credit. A candidate who selects four of five correct options in an extended multiple response item receives more credit than a candidate who selects two of five, even though neither achieves full marks. This partial credit mechanism means that thoughtful engagement with every option — carefully evaluating each rather than guessing on the ones that are unclear — directly improves the score contribution of NGN items even when complete accuracy is not achievable. For these NCLEX question types, there is no clinical reasoning benefit to leaving options unevaluated.
What Partial Credit Means for Preparation
The partial credit scoring of NGN NCLEX question types has a direct implication for how these formats should be practiced: the development goal is not simply to identify the clearly correct options quickly but to accurately evaluate every option including the ambiguous ones. Preparation that rushes through extended multiple response or matrix items to select the most obvious correct options and move on is leaving partial credit on the table. Preparation that applies independent evaluation to every option — including those that require genuine clinical reasoning to determine — is building the engagement habit that maximizes partial credit on exam day. This is why the independent yes-or-no evaluation habit is specifically important for NGN NCLEX question types: it prevents the tendency to evaluate only the clearly correct and clearly incorrect options while skipping the genuinely ambiguous ones that partial credit scoring specifically rewards engagement with.
Unfolding Case Study Scoring Independence
Each of the six questions in an unfolding case study is scored independently using standard NCLEX scoring — a correct answer on question three does not depend on whether question two was answered correctly. This independence has an important preparation implication: a reasoning error on one question within the set does not cascade into errors on subsequent questions unless the candidate allows their confidence about the previous answer to contaminate their reasoning on the next. The correct approach is to treat each question in an unfolding case study set as a fresh clinical judgment decision based on the current state of the scenario, without reference to previous answers. If question two is answered with uncertainty, question three should be approached with the same clinical rigor as if question two had been answered confidently — because the scoring of question three is entirely independent of question two’s outcome.
Preparing for All NCLEX Question Types: A Three-Week Integration Plan
Many candidates spend the majority of their preparation time on traditional NCLEX question types and add NGN practice only in the final days before the exam. This approach consistently underperforms a preparation strategy that integrates all NCLEX question types from the beginning — not because NGN formats require more total preparation time, but because format familiarity and cognitive habit development require distributed practice rather than concentrated last-minute exposure.
Week One: Format Orientation Before Clinical Reasoning Practice
The first week of preparation for all NCLEX question types should include a dedicated format orientation session — not a scored practice session but a structural familiarization session. Complete the official NCSBN NGN sample questions available at ncsbn.org: these are the only definitively accurate representations of how each NGN NCLEX question type looks and functions on the actual exam. Work through each format type deliberately, focusing on understanding the structural requirements — where to click in a hot spot item, how the bow tie sections are laid out, how the matrix grid functions — before worrying about whether the clinical content answers are correct. Platform familiarity reduces the cognitive load during actual exam sessions by removing format-decoding from the reasoning process. After the orientation session, all subsequent practice can focus on clinical reasoning within each format rather than on simultaneously decoding the format and reasoning through the clinical scenario.
Week Two and Three: Integrated Format Practice
From week two onward, every NCLEX practice question session should include a representative mix of all NCLEX question types — not all traditional or all NGN but a distribution that reflects the actual exam’s format integration. Within each session, apply the format-specific engagement strategy to each question type as it appears: two-read discipline and framework sequence for traditional multiple choice, independent yes-or-no for SATA and extended multiple response, center-first for bow tie, row-by-row for matrix, full document read before selecting for enhanced hot spot, CJMM skill identification before answering for unfolding case study questions. These format-specific habits must be built through consistent repetition rather than described during preparation and then applied cold on exam day. Three weeks of integrated practice is the minimum needed to make format-specific engagement habits automatic rather than effortful under exam pressure.
The Format-Specific Accuracy Tracking Rule
Throughout preparation, track accuracy separately for each of the NCLEX question types rather than monitoring only overall accuracy. A candidate with 62 percent overall accuracy who has 71 percent traditional format accuracy and 48 percent NGN format accuracy has a specific preparation gap that the overall number obscures. The same granularity applies within NGN formats — some candidates perform strongly on extended multiple response but struggle with bow tie; others find matrix items straightforward but find unfolding case study temporal reasoning difficult. Format-specific accuracy tracking reveals these patterns in time to address them before exam day. If a specific NCLEX question type consistently produces below-50-percent accuracy despite three weeks of integrated practice, that format needs a dedicated session of deliberate, format-specific clinical reasoning work — applying the engagement strategy explicitly to every question of that type — rather than continued mixed-format practice that dilutes the targeted attention the format requires.
- Official NGN sample questions: Complete the NCSBN official NGN sample questions at ncsbn.org at the beginning of preparation for definitive format orientation, and return to them in the final week as a calibration check. No third-party NCLEX question types platform fully replicates the official format — the NCSBN samples are the authoritative standard.
- Format-specific error logging: In the reasoning error log, record the NCLEX question type alongside the content category and error type for every incorrect answer. This produces format-specific error patterns that may reveal systematic engagement errors in specific formats rather than content knowledge gaps.
- Timed format exposure: Include at least one of each NGN NCLEX question type in every timed practice session from week two onward. Timed practice with all formats builds the pacing comfort that prevents NGN formats from consuming disproportionate exam time on the actual test day.
Common Mistakes Candidates Make With Specific NCLEX Question Types
Beyond general preparation gaps, specific NCLEX question types produce predictable engagement errors that appear consistently across candidates regardless of content knowledge level. Knowing these errors before they occur is the most efficient way to prevent them.
- Multiple choice — selecting the comprehensive option: Candidates frequently select the option that addresses the most concerns or describes the most thorough nursing response rather than the option that addresses the single highest priority. NCLEX question types reward targeted, prioritized responses over comprehensive ones. When four options all seem clinically reasonable, the correct one is the most specific to the highest clinical priority at the correct nursing process step.
- SATA — including options out of uncertainty: A common SATA error is including an option because it seems plausible rather than because independent evaluation confirms it is clinically applicable. Every option that is not clearly correct should be excluded. The uncertainty-inclusion error is more costly than the uncertainty-exclusion error on traditional all-or-nothing SATA scoring.
- Unfolding case study — re-reading the full scenario for every question: Candidates who re-read the entire scenario introduction for each of the six questions consume two to three times the necessary reading time on this NCLEX question type without improving clinical reasoning quality. Read the scenario fully for question one, then read only the newly added clinical information before subsequent questions.
- Bow tie — attempting all three sections simultaneously: Candidates who try to identify the central condition, nursing actions, and monitoring parameters at the same time create a circular reasoning loop that takes longer and produces less accurate selections than the sequential center-first approach. Commit to the center condition before touching the action or monitoring sections.
- Matrix — jumping between rows mid-completion: Candidates who jump between rows without completing each row in sequence lose track of which cells have been evaluated and either skip cells or re-evaluate cells already completed. Complete all column selections for row one before moving to row two, proceeding strictly in sequence.
- Enhanced hot spot — scanning for familiar terms: Candidates who scan the clinical document rather than reading it fully before selecting often miss the clinically significant term or phrase because it is embedded in a less prominent part of the document. Read the full document first, then select — the correct answer in enhanced hot spot NCLEX question types is often not the most visually prominent term.
Conclusion
NCLEX question types in 2026 span a broader cognitive range than at any previous point in the exam’s history — from the familiar four-option multiple choice question that has been part of the exam for decades to the six-question unfolding case study that tests all six CJMM clinical judgment cognitive skills within a single evolving patient scenario. Each format type exists for a specific reason: to measure a clinical competency that the other formats cannot measure with equivalent precision. Format familiarity converts that variety from a source of exam-day anxiety into a predictable cognitive landscape that candidates can navigate confidently. Master the traditional NCLEX question types through the two-read discipline, action verb identification, clinical reasoning framework application, and independent option evaluation. Master the NGN question types through CJMM skill identification, center-first bow tie commitment, independent yes-or-no evaluation for extended multiple response and matrix items, and full document reading for enhanced hot spot. Complete the NCSBN official NGN samples at the beginning of preparation for format orientation and return to them in the final week for calibration. Track format-specific accuracy separately throughout preparation and address format-specific gaps with targeted practice. Walk into the testing center knowing not just what to answer but how to engage every NCLEX question type that will appear — and the variety of formats becomes a competency demonstration rather than an obstacle.