NCLEX critical care nursing is a high-yield content area that challenges candidates not primarily because the clinical information is obscure but because the questions require a level of physiological specificity and clinical reasoning precision that routine content review often does not achieve. A candidate who understands in general terms that low cardiac output is bad and that vasopressors raise blood pressure will struggle with NCLEX critical care nursing questions that require distinguishing which vasopressor mechanism is appropriate for which shock physiology, what specific hemodynamic parameter indicates deterioration versus improvement, and what priority nursing assessment precedes any intervention in a critically ill patient whose condition could have multiple simultaneous explanations.
The NCLEX does not test critical care nursing as a specialty examination — it tests the entry-level nursing competencies that any registered nurse needs when caring for the acutely deteriorating patient in any clinical setting, not only the ICU. This means that NCLEX critical care nursing content appears in scenarios involving post-operative patients whose hemodynamics are shifting, patients on medical floors whose respiratory status is deteriorating, and emergency department patients presenting in undifferentiated shock. The clinical reasoning the NCLEX critical care nursing questions test — recognizing the specific pattern of physiological deterioration, analyzing what it indicates, prioritizing the hypotheses by urgency, and identifying the correct first nursing action — is the same clinical judgment that the NCSBN identified as the core competency for safe entry-level nursing practice.
This guide covers the highest-yield NCLEX critical care nursing content across six core clinical areas: hemodynamic monitoring and interpretation, shock recognition and management, mechanical ventilation nursing priorities, acute respiratory distress syndrome, post-operative critical care, and critical care pharmacology. For each area, the focus is on the specific clinical distinctions, priority assessment principles, and nursing action sequences that appear most consistently on the exam — not comprehensive critical care nursing theory but the precise clinical knowledge and reasoning that produces correct answers on the most demanding NCLEX critical care nursing questions.
Hemodynamic Monitoring: Parameters, Trends, and Nursing Priorities
Hemodynamic monitoring is the foundation of NCLEX critical care nursing — the clinical measurement framework that provides the physiological data needed to distinguish shock types, evaluate intervention effectiveness, and identify deterioration before it becomes irreversible.
The Key Hemodynamic Parameters
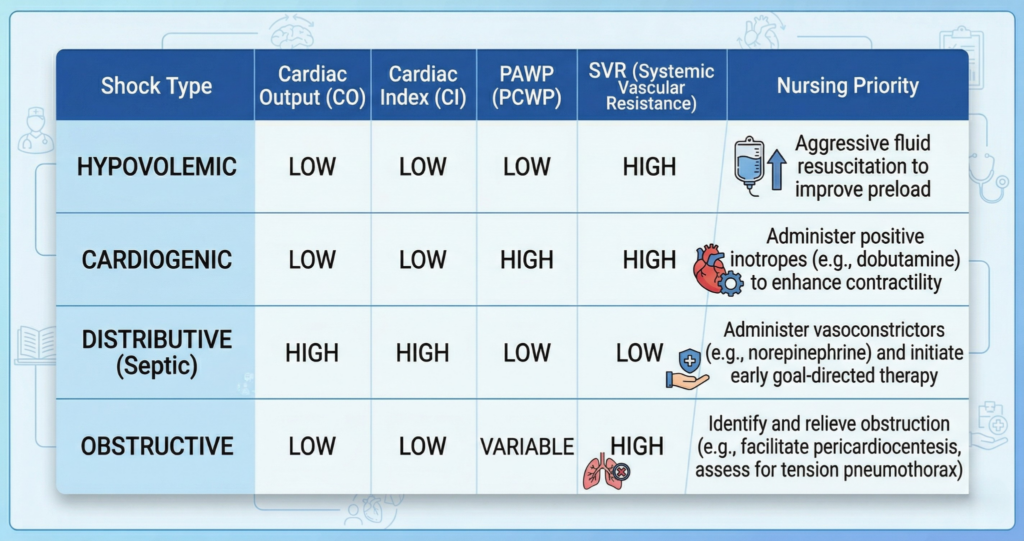
NCLEX critical care nursing questions on hemodynamic monitoring test whether candidates can interpret the clinical significance of specific parameter values and trends rather than simply recall normal ranges. Cardiac output is the volume of blood the left ventricle ejects per minute — normal is 4 to 8 liters per minute — and is the fundamental indicator of circulatory adequacy. Cardiac output divided by body surface area produces the cardiac index — normal 2.5 to 4.0 L/min/m squared — which is the parameter that adjusts cardiac output for body size and makes comparison across patients clinically valid. Systemic vascular resistance reflects the afterload the left ventricle works against to eject blood — normal is 800 to 1200 dynes/sec/cm5. Pulmonary artery wedge pressure reflects left ventricular preload — the volume filling the left ventricle — and is the most direct available measure of left-sided filling pressure in critically ill patients who cannot be reliably assessed by clinical examination alone. The NCLEX critical care nursing interpretation framework for these parameters is the relationship between them: high SVR with low cardiac output indicates cardiogenic or obstructive shock physiology; low SVR with high cardiac output indicates distributive shock physiology; low filling pressures across the board indicate hypovolemic physiology.
Arterial Line Nursing: Assessment and Complication Prevention
Arterial line management is a high-yield NCLEX critical care nursing nursing skill that tests both monitoring interpretation and complication prevention. The arterial line provides continuous blood pressure monitoring and arterial blood gas sampling without repeated punctures. The NCLEX critical care nursing priority assessment for an arterial line is the neurovascular check of the extremity distal to the insertion site — checking capillary refill, color, warmth, sensation, and movement. Arterial lines are placed in high-pressure arterial circulation; disconnection produces rapid blood loss, making securing all connections and maintaining the pressure bag at 300 mmHg the highest-priority safety checks at every assessment. A dampened waveform — one that appears low and blunted rather than the sharp systolic peak — indicates clot at the catheter tip, air in the line, or catheter malposition, and requires immediate troubleshooting including flushing the line with the pressurized saline flush before calling the provider. Never aspirate from a dampened arterial line without provider guidance.
Central Venous Catheter: Insertion Complications and Ongoing Care
Central venous catheter complications are a consistent NCLEX critical care nursing topic tested at the highest difficulty levels because they require the ability to identify complications from clinical findings rather than from explicit complication labeling. Pneumothorax from subclavian or internal jugular CVC insertion presents with sudden dyspnea, decreased or absent breath sounds unilaterally, and tracheal deviation away from the affected side in tension pneumothorax — requiring immediate chest X-ray before any fluids are administered through the new line. Air embolism — from disconnection of the line or from the insertion process — presents with sudden chest pain, dyspnea, hypotension, and a churning machinery murmur audible at the precordium. The NCLEX critical care nursing emergency response for suspected air embolism is placing the patient in Trendelenburg position with the left side down — trapping air in the right ventricle away from the pulmonary outflow tract — and immediate provider notification. CVC-associated bloodstream infection prevention requires aseptic technique during all access events, daily assessment of the need for the line, and dressing changes per protocol.
Shock Recognition and Management: The Four Types and Their Distinctions

Shock is the most consistently tested NCLEX critical care nursing topic because it appears in scenarios across every body system and because the correct nursing response depends on correctly identifying the shock type — interventions appropriate for one type can be harmful in another.
Hypovolemic Shock: Fluid Loss and Replacement Priorities
Hypovolemic shock results from inadequate circulating volume — from hemorrhage, severe dehydration, burns, or third-spacing of fluid. The NCLEX critical care nursing clinical progression is predictable and must be recognized across its stages. Class I hemorrhage (less than 750 mL, less than 15% blood volume): heart rate below 100, blood pressure normal, respiratory rate normal. Class II (750 to 1500 mL, 15 to 30%): heart rate 100 to 120, blood pressure normal to slightly decreased, anxiety, and importantly, narrowing pulse pressure — systolic maintained by increasing SVR while diastolic rises. Class III (1500 to 2000 mL, 30 to 40%): heart rate above 120, blood pressure decreased, respiratory rate 30 to 40, altered mental status. Class IV (more than 2000 mL, more than 40%): heart rate above 140, blood pressure severely decreased, unconsciousness. The NCLEX critical care nursing tachycardia-as-earliest-sign principle is critical — blood pressure is preserved through compensatory vasoconstriction until class III hemorrhage, making tachycardia the more sensitive early indicator. Initial management is two large-bore peripheral IV lines and isotonic crystalloid resuscitation while blood products are being prepared for hemorrhagic shock.
Cardiogenic Shock: Pump Failure Management
Cardiogenic shock results from the heart’s failure to generate adequate cardiac output despite normal or elevated filling pressures — the pump is failing, not the volume. NCLEX critical care nursing presentation is cold, clammy, pale extremities from compensatory vasoconstriction, hypotension, tachycardia, pulmonary crackles from left-sided back-pressure into the pulmonary circulation, and elevated central venous pressure from right-sided back-pressure. The critical clinical distinction from hypovolemic shock in NCLEX critical care nursing is the pulmonary edema — hypovolemic shock produces dry lungs from low filling pressures; cardiogenic shock produces wet lungs from high filling pressures. Management priorities in cardiogenic shock are carefully titrated inotropes to improve contractility, vasopressors to maintain perfusion pressure, and judicious diuretics if pulmonary edema is severe — but not aggressive fluid resuscitation, which would worsen the already-elevated filling pressures. Fluid administration in cardiogenic shock accelerates pulmonary edema and worsens the clinical picture — a critical NCLEX critical care nursing safety rule.
Distributive Shock: Septic, Anaphylactic, and Neurogenic
Distributive shock produces a paradoxical presentation in NCLEX critical care nursing scenarios — despite dangerously inadequate tissue perfusion, the patient appears warm, flushed, and vasodilated rather than cold and vasoconstricted. Massive vasodilation from inflammatory mediators (septic shock), histamine release (anaphylactic shock), or loss of sympathetic tone (neurogenic shock from spinal cord injury) distributes blood away from vital organs despite normal or high cardiac output. The NCLEX critical care nursing distinctions between distributive subtypes: septic shock requires the one-hour bundle (cultures before antibiotics, broad-spectrum antibiotics within one hour, IV fluid bolus 30 mL/kg crystalloid, vasopressors for refractory hypotension after fluid resuscitation, serum lactate). Anaphylactic shock requires epinephrine IM as the absolute first-line intervention — not antihistamines, not corticosteroids as the first action — with epinephrine’s alpha-1 and beta-2 receptor actions reversing both the vasodilation and the bronchospasm simultaneously. Neurogenic shock from high spinal cord injury presents uniquely with bradycardia alongside hypotension — the opposite of all other shock types — because loss of sympathetic tone removes the compensatory tachycardia mechanism.
Obstructive Shock: Tension Pneumothorax and Cardiac Tamponade
Obstructive shock occurs when a mechanical impedance to blood flow prevents adequate cardiac output despite normal pump function and adequate volume. The two highest-yield NCLEX critical care nursing obstructive shock scenarios are tension pneumothorax and cardiac tamponade. Tension pneumothorax presents with tracheal deviation away from the affected side, absent breath sounds unilaterally, jugular venous distension, severe respiratory distress, and hemodynamic collapse — requiring immediate needle decompression at the second intercostal space, midclavicular line before chest X-ray is obtained. Cardiac tamponade presents with Beck’s triad: hypotension, jugular venous distension, and muffled heart sounds. It most commonly occurs after cardiac surgery, penetrating chest trauma, or pericarditis. Emergency management is pericardiocentesis. The shared NCLEX critical care nursing feature of both conditions is JVD alongside hypotension — the elevated venous pressure from impaired right heart filling is the diagnostic clue that distinguishes obstructive from hypovolemic shock.
Mechanical Ventilation: Nursing Priorities and Alarm Management
Mechanical ventilation nursing is among the most technically specific NCLEX critical care nursing content areas — and among the most consistently tested because it requires understanding of both the physiological rationale for ventilator settings and the nursing response to ventilator alarms and complications.
Ventilator Modes and Basic Settings
NCLEX critical care nursing ventilator questions test the nursing implications of basic ventilator settings rather than the technical mechanics of mode selection, which is the provider’s domain. Tidal volume — the volume of each delivered breath — is typically set at 6 to 8 mL per kilogram of ideal body weight in lung-protective ventilation strategies, which reduce ventilator-induced lung injury in conditions like ARDS. Respiratory rate, PEEP (positive end-expiratory pressure), and FiO2 (fraction of inspired oxygen) are the four parameters the NCLEX critical care nursing nurse monitors most closely. PEEP keeps alveoli open at end-expiration, recruits collapsed alveolar units, improves oxygenation in diffuse lung injury, and reduces the work of breathing — but excessive PEEP reduces venous return and can decrease cardiac output. The NCLEX critical care nursing PEEP monitoring priority is hemodynamic: a patient whose PEEP is increased to improve oxygenation must be monitored for blood pressure decrease and tachycardia indicating reduced preload from impaired venous return.
Ventilator Alarms: The Priority Response Sequence
Ventilator alarm response is the highest-yield mechanical ventilation topic in NCLEX critical care nursing — tested through scenarios that present a ventilated patient with a specific alarm and clinical findings and ask what the nurse does first. The universal priority response to any ventilator alarm in which the patient appears in distress is the same sequence applied before any alarm-specific troubleshooting: manually ventilate the patient with a bag-valve-mask device at 100 percent oxygen while the alarm cause is identified. This sequence ensures that the patient receives adequate oxygenation and ventilation during the period of alarm investigation rather than waiting for troubleshooting to be completed before ventilation is restored. High pressure alarms indicate increased resistance to breath delivery — causes include secretion accumulation, bronchospasm, patient coughing or biting the tube, and kinked ventilator tubing. Low pressure alarms indicate loss of circuit integrity — causes include disconnection, cuff leak, or chest tube with large air leak. Low minute ventilation alarms indicate inadequate total ventilation — causes include shallow breathing, circuit disconnection, or cuff leak. The NCLEX critical care nursing response sequence for every alarm: manually ventilate with BVM first, identify the alarm cause second, correct the cause third, reconnect to ventilator when patency and function are confirmed.
Endotracheal Tube Care and Complications
Endotracheal tube care nursing priorities in NCLEX critical care nursing center on tube security, cuff management, and aspiration prevention. The ETT cuff must maintain a seal adequate to prevent aspiration but not so tight as to cause tracheal pressure injury — cuff pressure is measured and maintained between 20 and 30 cmH2O. Cuff pressure above 30 cmH2O causes tracheal mucosal ischemia and necrosis. Below 20 cmH2O, micro-aspiration of oral secretions past the cuff occurs, which is the primary mechanism of ventilator-associated pneumonia. VAP prevention bundle priorities in NCLEX critical care nursing are: maintain head of bed elevation at 30 to 45 degrees, daily sedation vacations with readiness-to-wean assessment, daily oral hygiene with chlorhexidine, subglottic suctioning if available, and stress ulcer and DVT prophylaxis. Accidental extubation is the most urgent ETT complication — requiring immediate manual ventilation with BVM, immediate provider notification, and preparation for emergent reintubation while monitoring for hypoxia.
ARDS: Recognition, Ventilator Strategy, and Nursing Priorities
Acute respiratory distress syndrome is one of the highest-yield NCLEX critical care nursing diagnoses because it combines complex pathophysiology, specific ventilator management principles, and high-acuity nursing assessment that is consistently tested at the most difficult question levels.
ARDS Pathophysiology and Berlin Criteria
ARDS pathophysiology in NCLEX critical care nursing begins with widespread alveolar inflammation and damage from a triggering insult — most commonly sepsis, pneumonia, aspiration, trauma, or massive transfusion. The inflammatory cascade damages the alveolar-capillary membrane, causing increased permeability and flooding of alveoli with protein-rich fluid rather than air. The result is diffuse bilateral infiltrates on chest X-ray, severe hypoxemia that does not fully respond to supplemental oxygen (the shunt physiology of non-aerated, perfused alveoli), and reduced lung compliance. The Berlin criteria for ARDS diagnosis require: onset within one week of a clinical insult, bilateral opacities on chest imaging not fully explained by cardiac failure or fluid overload, and hypoxemia defined by the PaO2/FiO2 ratio. Mild ARDS is a P/F ratio of 200 to 300 on PEEP at least 5 cmH2O; moderate ARDS is 100 to 200; severe ARDS is below 100. The NCLEX critical care nursing P/F ratio is the diagnostic tool that quantifies the severity of gas exchange impairment — normal P/F ratio is above 400.
Lung-Protective Ventilation Strategy
The lung-protective ventilation strategy for ARDS is the most specific NCLEX critical care nursing ventilator management principle and is consistently tested because it appears counterintuitive. Low tidal volumes of 6 mL/kg ideal body weight — lower than the historical 10 to 15 mL/kg standard — reduce ventilator-induced lung injury by preventing overdistension of the relatively healthy alveoli that remain in an ARDS lung whose injured sections are collapsed and unable to participate in ventilation. The remaining open alveoli receive the full tidal volume meant for the entire lung, making them vulnerable to overdistension injury at normal tidal volumes. Higher PEEP levels recruit collapsed alveoli and maintain their patency, improving the gas exchange surface area and reducing the shunt fraction. The nursing implication of high PEEP in ARDS is the same as in all NCLEX critical care nursing PEEP scenarios: monitor hemodynamic parameters for the venous return impairment that high PEEP can produce, and report blood pressure decrease or tachycardia to the provider.
Prone Positioning in ARDS
Prone positioning is a high-yield NCLEX critical care nursing intervention for severe ARDS that significantly improves oxygenation in patients who do not respond adequately to standard lung-protective ventilation. Placing the patient face-down redistributes the consolidated, fluid-filled lung tissue from the dependent (posterior) zones — where it restricts ventilation in supine patients — to the anterior zones, allowing the now-dependent posterior zones to be recruited by PEEP and gravity. The oxygenation improvement in prone positioning is typically significant and rapid. The NCLEX critical care nursing nursing priorities for prone positioning are: adequate staff for safe repositioning (typically five or more nurses), securing all lines and devices before turning, padding all pressure points (face, chest, pelvis, knees) to prevent pressure injury, maintaining the endotracheal tube and all vascular access lines in secure, accessible positions, and monitoring for facial edema that accumulates during prolonged prone sessions. Prone positioning is typically maintained for 16 or more continuous hours per session in severe ARDS protocols.
Post-Operative Critical Care: Highest-Risk Assessment Priorities
Post-operative critical care is one of the most clinically versatile NCLEX critical care nursing content areas because post-operative patients can deteriorate through multiple simultaneous pathways — hemorrhage, respiratory depression, fluid shifts, cardiac events, and infection — and the nursing assessment must be comprehensive enough to detect the most immediately dangerous among them.
Immediate Post-Operative Assessment Sequence
The universal immediate post-operative assessment sequence in NCLEX critical care nursing follows the ABCs with additional systematic elements: airway patency and ability to protect the airway, respiratory rate and quality including breath sounds, hemodynamic status including heart rate and blood pressure with comparison to pre-operative baseline, surgical site assessment including dressing integrity and any drainage characteristics, level of consciousness and orientation, pain assessment, and IV site and fluid status review. The NCLEX critical care nursing priority among these assessments when the post-operative patient presents with multiple simultaneous findings is always respiratory first: anesthesia and opioid analgesics both cause respiratory depression, and a patient with a respiratory rate below 12 or oxygen saturation below 94 percent in the immediate post-operative period requires immediate intervention before any other assessment continues. The second priority is hemodynamic — tachycardia in the post-operative patient is the earliest sign of hemorrhage, pain, hypovolemia, or infection and requires systematic investigation rather than symptom treatment.
Post-Operative Hemorrhage: Recognition and Response
Post-operative hemorrhage recognition is a critical NCLEX critical care nursing skill because early hemorrhage often presents subtly — through vital sign changes rather than obvious bleeding. The hemorrhage recognition sequence is tachycardia first (the compensatory mechanism that maintains blood pressure as volume falls), followed by narrowing pulse pressure (systolic maintained, diastolic rises from SVR compensation), followed by blood pressure drop (late finding indicating decompensation). Surgical site findings that indicate bleeding include increasing saturation of the dressing, drainage that is brighter red than expected or increasing in volume rather than decreasing, and distension of body cavities that would receive internal blood — abdominal rigidity and distension after abdominal surgery, neck swelling after thyroid or carotid surgery, thigh swelling after orthopedic surgery. The NCLEX critical care nursing response to suspected post-operative hemorrhage is: maintain IV access with large-bore lines, apply direct pressure to accessible wounds, notify the surgeon immediately, position for hemodynamic support, and prepare for blood transfusion and possible return to the operating room.
Specific High-Risk Post-Operative Populations
Several post-operative populations have NCLEX critical care nursing priority assessments that are condition-specific and represent consistently tested high-yield content. Post-cardiac surgery patients: mediastinal tube drainage greater than 200 mL per hour for two consecutive hours indicates hemorrhage requiring immediate provider notification; sudden cessation of previously brisk drainage indicates possible clot obstruction with cardiac tamponade risk, not improvement. Post-thyroid surgery patients: laryngeal edema and airway compromise from tracheal pressure or bleeding into the surgical site, hypocalcemia from inadvertent parathyroid removal presenting as tingling, tetany, positive Chvostek and Trousseau signs. Post-nephrectomy patients: urine output monitoring as the primary indicator of remaining kidney function with a minimum target of 0.5 mL/kg/hour. Post-thoracotomy patients: chest tube patency and fluctuation — water-seal fluctuation (tidaling) with respirations confirms patency, cessation of fluctuation may indicate occlusion, excessive bubbling in the water seal indicates persistent air leak.
Critical Care Pharmacology: High-Stakes Medications and Nursing Priorities
Critical care pharmacology is among the most technically demanding NCLEX critical care nursing content areas because the medications used in critical illness are potent, have narrow therapeutic windows, and require specific nursing assessment sequences that differ from general pharmacology safety principles.
Vasopressors and Inotropes: Mechanism and Monitoring
Vasopressor and inotrope pharmacology is the highest-yield NCLEX critical care nursing pharmacology topic. Norepinephrine is the first-line vasopressor for septic shock — its primary alpha-1 receptor activity produces vasoconstriction that raises blood pressure and systemic vascular resistance, with secondary beta-1 activity providing mild positive inotropy. Dopamine at high doses (10 to 20 mcg/kg/min) provides alpha-1 and beta-1 effects for combined vasopressor and inotropic support. Dobutamine is a selective beta-1 agonist providing positive inotropy and mild vasodilation — used in cardiogenic shock to improve contractility without the vasoconstriction that would further increase afterload on the failing heart. Vasopressin is used as a second-line vasopressor in septic shock, acting through V1 receptors to produce vasoconstriction independent of adrenergic mechanisms. The NCLEX critical care nursing priority monitoring for all vasopressors is continuous hemodynamic monitoring — blood pressure via arterial line, heart rate, and urine output as an organ perfusion indicator — with titration based on mean arterial pressure target (typically MAP above 65 mmHg in septic shock) rather than systolic blood pressure alone.
Anticoagulation in Critical Care
Anticoagulation management is a consistently tested NCLEX critical care nursing pharmacology area because it requires balancing therapeutic benefit against bleeding risk in patients who are already physiologically vulnerable. Heparin infusions in critical care are titrated to aPTT values of 60 to 100 seconds, with dose adjustments based on institutional weight-based heparin protocol. The NCLEX critical care nursing heparin safety priority is bleeding assessment: monitoring for new-onset bleeding from IV sites, neurological changes suggesting intracranial hemorrhage, hematuria, and change in level of consciousness. Heparin-induced thrombocytopenia — an immune-mediated complication producing paradoxical thrombosis from platelet-activating antibodies — is recognized by a 50 percent or greater platelet count drop from baseline at 5 to 10 days after heparin initiation, accompanied by new thrombotic events. HIT management requires immediate heparin discontinuation and initiation of a non-heparin anticoagulant — argatroban or bivalirudin — because the underlying immune mechanism persists even after heparin is stopped and alternative anticoagulation is required.
Sedation and Analgesia in Mechanically Ventilated Patients
Sedation and analgesia management for mechanically ventilated patients is a high-yield NCLEX critical care nursing area because it requires the integration of comfort, safety, and delirium prevention goals. The analgesia-first approach — addressing pain before sedation — is the current standard because unrelieved pain drives agitation, requiring higher sedation doses that increase complications. The Richmond Agitation-Sedation Scale (RASS) targets for most mechanically ventilated patients are 0 (alert and calm) to -2 (light sedation, briefly awakened with voice), with avoidance of deep sedation except in specific clinical indications such as elevated ICP management or severe ARDS requiring prone positioning. Daily sedation vacations — scheduled interruption of sedation infusions with assessment of spontaneous awakening — reduce total sedation exposure, reduce ventilator duration, and reduce ICU length of stay. The NCLEX critical care nursing priority during a sedation vacation is close monitoring for respiratory distress, hemodynamic instability, and patient self-extubation, with clear criteria for restarting sedation if the patient does not tolerate the trial.
- Propofol in critical care: Propofol infusion syndrome is a rare but potentially fatal complication of high-dose prolonged propofol infusions, presenting as metabolic acidosis, rhabdomyolysis, cardiac dysrhythmias, and renal failure. NCLEX critical care nursing monitoring includes daily serum triglycerides (propofol is lipid-based), serum lactate for metabolic acidosis, and creatinine kinase for rhabdomyolysis — with immediate provider notification for any of these laboratory abnormalities.
- Neuromuscular blocking agents: NMBAs such as cisatracurium produce complete skeletal muscle paralysis to facilitate mechanical ventilation in the most severe ARDS cases. NCLEX critical care nursing safety requirements during NMBA infusions are absolute: train-of-four peripheral nerve stimulation monitoring to assess depth of blockade, mandatory concurrent sedation and analgesia (NMBAs provide no sedation or analgesia and conscious paralysis is a critical harm event), eye care to prevent corneal injury from the abolished blink reflex, and pressure injury prevention from the inability to reposition.
Conclusion
NCLEX critical care nursing is not a specialty examination — it is an entry-level clinical reasoning examination applied to the highest-acuity scenarios that any registered nurse may encounter in any clinical setting. The hemodynamic monitoring parameters that distinguish shock types, the ventilator alarm response sequence that prioritizes BVM ventilation before troubleshooting, the ARDS lung-protective ventilation principles, the post-operative assessment sequence that prioritizes respiratory then hemodynamic status, and the vasopressor mechanisms that match specific shock physiologies — these are the clinical reasoning chains that NCLEX critical care nursing questions test, not the ability to operate ICU equipment or manage complex monitoring systems.
Study NCLEX critical care nursing through condition-to-intervention reasoning chains: for each clinical scenario, practice generating from memory the pathophysiology that produces the clinical findings, the hemodynamic pattern that distinguishes this condition from similar presentations, the priority nursing assessment before any intervention, and the first-line intervention with its nursing monitoring requirements. Active recall of these reasoning chains — closing notes and generating the complete clinical sequence from memory — produces the application-level competency that NCLEX questions require. The critical care content that appears most daunting before preparation reveals its internal logic clearly once the pathophysiology-to-nursing-action chains are understood rather than memorized as disconnected facts.