The most frustrating NCLEX experience is not the not-passing result itself — it is the experience of receiving a not-passing result while genuinely believing you were prepared. Hours of daily study. Thousands of NCLEX practice questions completed. Content reviewed comprehensively. Practice session accuracy that felt adequate. And still a not-passing result that reveals a gap between preparation investment and examination performance that the candidate did not see coming and cannot immediately explain.
Understanding the most common reasons students fail the NCLEX requires looking past the obvious explanation — insufficient preparation — to the specific mechanisms by which well-intentioned, high-effort preparation produces inadequate clinical reasoning development. The majority of candidates who do not pass the NCLEX on their first attempt are not candidates who did not try hard enough. They are candidates whose preparation approach was misaligned with what the examination actually measures in ways that high preparation effort could not compensate for. A candidate who completes 3,000 NCLEX practice questions with answer-checking review has invested enormous preparation effort into a technique that extracts approximately 20 percent of the available clinical reasoning development from each question. A candidate who completes 1,000 NCLEX practice questions with full four-question rationale protocol extracts five times the clinical reasoning development per question. The first candidate has worked much harder. The second candidate has prepared much more effectively.
This guide identifies the eight most common reasons students fail the NCLEX — organized not as general advice about studying harder but as specific, mechanistic explanations of why each failure pattern occurs and what precise preparation change addresses each one. Every reason on this list is addressable. None of them requires exceptional intelligence, exceptional resources, or an exceptional amount of additional preparation time. They require specific preparation behavior changes that target the actual mechanism of each failure pattern rather than the generic additional effort that most candidates instinctively reach for after a not-passing result.
Reason 1: Answer-Checking Instead of Rationale Analysis
The Failure Mechanism
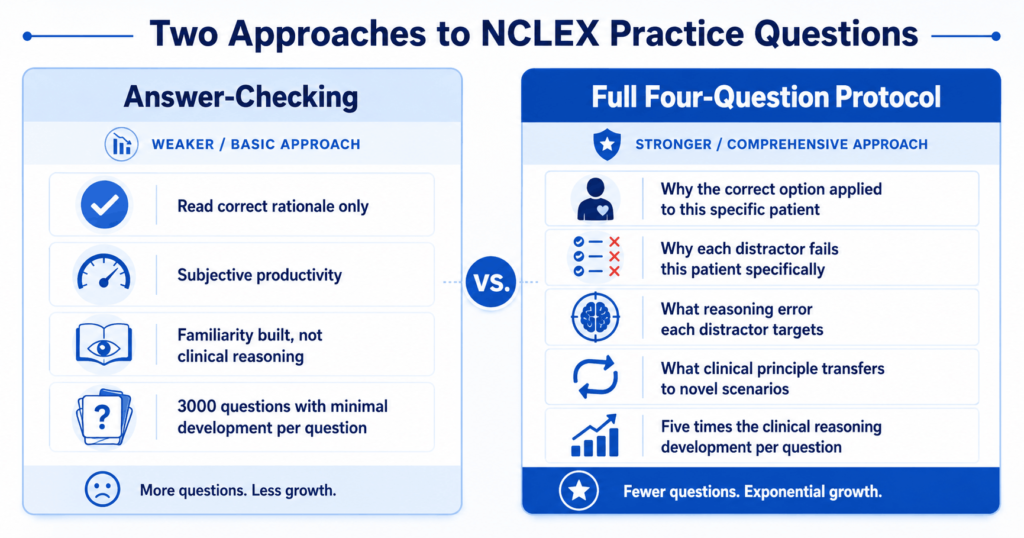
The most common reason students fail the NCLEX despite completing thousands of NCLEX practice questions is answer-checking — reading the correct answer’s rationale and moving to the next question without applying the full analytical protocol that extracts the maximum clinical reasoning value from each question. Answer-checking produces the subjective experience of productive preparation: questions are being completed, correct answers are being confirmed, rationales are being read. But the clinical reasoning development that actually builds the competency the NCLEX measures occurs through the complete four-question rationale analysis — not through confirmation of the correct answer alone. A student who reads the correct answer’s rationale is learning what the right answer is. A student who analyzes why each incorrect option fails for this specific patient, what reasoning error would lead to each distractor selection, and what clinical principle the question transfers to new scenarios is learning how to reason correctly — which is what the examination tests.
The Specific Fix
Apply the complete four-question protocol to every NCLEX practice question regardless of whether it was answered correctly or incorrectly: what clinical principle does the correct answer apply to this specific patient, why does each incorrect option fail for this specific patient in this specific scenario (not in general, but for this patient), what reasoning error type would lead a candidate to select each distractor, and what clinical principle transfer does this question teach for future novel scenarios. This protocol takes approximately three to five minutes per question for a 50-question session — producing a 150 to 250 minute rationale review for a session that the answer-checking approach completes in 15 minutes. The additional time investment extracts five times the clinical reasoning development per question. A candidate who consistently applies this protocol to 1,000 NCLEX practice questions will outperform a candidate who completes 3,000 questions with answer-checking because the protocol builds the clinical judgment the examination measures rather than the familiarity that answer-checking builds.
Reason 2: Treating Every Wrong Answer as a Content Gap
The Failure Mechanism
The second most common reason students fail the NCLEX is the systematic misdiagnosis of incorrect NCLEX practice questions as content gaps requiring additional content review — when the majority of incorrect answers are produced by reasoning pattern errors that content review cannot fix. A candidate who misses a cardiovascular prioritization question because they selected the psychosocial option before the unaddressed physiological need does not have a cardiovascular knowledge gap. They have a priority framework application error that produces incorrect answers across every content area where psychosocial and physiological options appear simultaneously. Returning to cardiovascular content review after this error will not close the gap — because the gap is not cardiovascular content. The same reasoning error will reappear in the next cardiovascular question, and the next respiratory question, and the next neurological question, because the error is a cross-content reasoning pattern, not a content-specific knowledge deficiency.
The Specific Fix
Classify every incorrect NCLEX practice question by error type using the four-category framework before deciding on any preparation response. Knowledge gap: the clinical principle required for the correct answer was genuinely absent from the accessible knowledge base — content review is the correct response. Reasoning pattern error: the clinical content was present but misapplied — a specific behavioral correction applied to the identified pattern is the correct response, not content review. Patient context error: the correct clinical reasoning was applied to the wrong patient interpretation — deliberate stem reading practice with the physiological urgency scan is the correct response. NGN cognitive skill error: the wrong CJMM cognitive skill was applied to an NGN format question — skill-specific practice and action verb identification are the correct responses. Each error type has a specific, different preparation response. Applying content review to reasoning pattern errors produces preparation effort without preparation improvement — which is the most common mechanism by which high-effort preparation produces insufficient clinical reasoning development.
Reason 3: Completing NCLEX Practice Questions Without Timed Conditions
The Failure Mechanism
The third common reason students fail the NCLEX is preparing with untimed NCLEX practice questions and discovering at the actual examination that their clinical reasoning quality deteriorates significantly under the timing pressure they have never practiced. The NCLEX’s five-hour clock produces an average of approximately 90 seconds per question across the session length. A candidate who has consistently taken two to three minutes per question during preparation — because they take the time they need to reason carefully without any clock pressure — has calibrated their clinical reasoning process to a temporal framework that the examination does not accommodate. When the exam’s clock becomes real, the candidate must either rush their reasoning (producing quality deterioration) or run behind the time benchmark (producing increasing clock anxiety that degrades reasoning quality in the latter half of the session). Neither outcome reflects the candidate’s genuine clinical reasoning capacity — both are the direct consequence of preparation conducted without the time pressure that the actual examination imposes.
The Specific Fix
Conduct every NCLEX practice question session under timed conditions from the first day of preparation — not as an occasional simulation but as the standard for every session. Set a visible timer for 90 seconds per question and apply the milestone clock check at questions 25, 50, 75, and 100 of every simulated session to confirm pacing is on track. Initial timed practice sessions will feel rushed and may produce lower accuracy than untimed practice — this is expected and temporary. The clinical reasoning quality that emerges from consistent timed practice is calibrated to the examination’s actual temporal constraints, which means it remains available under exam conditions rather than being impaired by the novel timing demand the examination introduces. Within two to three weeks of consistent timed NCLEX practice questions, most candidates find that their reasoning quality under timed conditions approaches their untimed quality — because the timing has become a familiar preparation constraint rather than a novel exam-day stressor.
Reason 4: Ignoring NGN Format Until the Final Weeks
The Failure Mechanism
A fourth reason students fail the NCLEX in 2026 is deferring NGN-specific NCLEX practice questions until the final weeks of preparation — after the majority of preparation has been invested in traditional multiple choice format. The NGN clinical judgment formats (unfolding case study sets, bow tie questions, extended multiple response, matrix questions, and trend questions) test cognitive skills that traditional multiple choice practice does not develop: sustained narrative reasoning across developing patient scenarios, partial credit response strategy, and CJMM cognitive skill identification and application. A candidate who defers NGN format practice until week five of a six-week preparation period is attempting to develop these skills in one week that require at least four weeks of consistent deliberate practice to build to exam-ready fluency. With the April 2026 test plan’s increased NGN proportion, the performance cost of NGN underpreparation is higher than in any previous year — a below-standard NGN accuracy now contributes to a larger share of the ability estimate the CAT algorithm builds from the full response pattern.
The Specific Fix
Integrate NGN NCLEX practice questions as 30 to 35 percent of every practice session from the first day of preparation — not as a final-week addition but as a built-in daily proportion. Apply the CJMM action verb identification habit to every NGN question before reading any option: read the question stem, identify the action verb, name the cognitive skill it indicates (recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, evaluate outcomes), and use that skill identification to determine what the correct answer must demonstrate before option engagement. Complete unfolding case study question sets as full six-question sets with the carry-forward protocol applied between questions rather than practicing individual NGN items extracted from their case context. Track NGN accuracy separately from traditional format accuracy in every weekly micro-audit to confirm the NGN-specific preparation is producing the above-50-percent NGN benchmark required for readiness.
Reason 5: Using Low-Quality or Outdated Question Banks
The Failure Mechanism
A fifth reason students fail the NCLEX is selecting NCLEX practice questions from question banks that do not accurately reflect the current examination’s difficulty, format, or clinical reasoning complexity — and receiving a misleading accuracy signal that suggests readiness the actual examination then refutes. Low-quality question banks present questions at below-NCLEX difficulty that reward content recognition rather than clinical reasoning framework application — producing practice accuracy percentages in the 70 to 80 percent range that feel excellent relative to any reasonable preparation standard but that correspond to approximately 55 to 60 percent performance on a well-calibrated question bank. The candidate who completes weeks of preparation on a low-difficulty question bank arrives at the examination with an inflated readiness signal and without the clinical reasoning skills that the examination’s actual difficulty requires. Outdated question banks — resources created before the 2023 NGN launch or before the April 2026 test plan update — compound this problem by testing clinical content weightings and format proportions that the current examination has moved beyond.
The Specific Fix
Select a primary NCLEX practice questions platform that meets three specific quality criteria: it reflects the current April 2026 or later test plan (verifiable by the platform’s published content update documentation), it includes all five NGN format types with explicit CJMM framework alignment, and its question difficulty is calibrated to produce practice accuracy in the 55 to 65 percent range for well-prepared candidates — not the 70 to 80 percent range that indicates below-NCLEX difficulty. Calibrate your question bank’s difficulty against the NCSBN official NGN sample questions at ncsbn.org: if your practice accuracy on the official NCSBN samples is significantly higher or lower than on your question bank, the bank’s difficulty calibration does not match the current examination. The leading platforms with established current-examination calibration are UWorld, Kaplan, ATI, and the NCSBN Learning Extension — each with documented NGN content and current test plan alignment.
Reason 6: Preparation Without Recovery — The Burnout Mechanism

The Failure Mechanism
A sixth reason students fail the NCLEX is the preparation-without-recovery pattern that produces cognitive burnout in the final weeks of preparation — the period when clinical reasoning quality is most critical. Candidates who maintain peak-intensity NCLEX practice questions sessions seven days per week without designated recovery days accumulate a cognitive deficit that progressively degrades the quality of each subsequent session: declining ability to engage rationale review analytically, increasing difficulty concentrating through a full question set, and the emotional flatness that accompanies physiological depletion. This degradation is invisible in the question volume metrics that candidates typically use to track preparation — a candidate can complete the same 50 NCLEX practice questions per day in week five as in week one, producing the same session volume with approximately half the clinical reasoning development per question as cognitive fatigue reduces the analytical quality of each session. The candidate arrives at the examination physiologically and cognitively depleted — attempting to demonstrate clinical reasoning competency with a nervous system whose primary cognitive capacities are impaired.
The Specific Fix
Build two non-preparation days per week into the NCLEX practice questions schedule as non-negotiable infrastructure rather than optional rest. Apply a 90-minute maximum session length for intensive practice question sessions — clinical reasoning quality declines measurably after 90 minutes of intensive engagement, and continuing beyond this point produces question completion without meaningful clinical reasoning development. Apply the final-week taper: the week before the examination is a calibration week, not a peak-intensity week. The final simulation is completed seven days before the exam. Daily question volume decreases progressively across the final week. The two days before the exam include only brief Anki spaced repetition review. Exam morning includes no practice questions at all. This taper allows the cognitive capacity built across the preparation period to consolidate and recover into its most accessible state for exam day rather than arriving at the examination in a state of accumulated depletion.
Reason 7: Misreading the Practice Accuracy Signal
The Failure Mechanism
A seventh reason students fail the NCLEX is misinterpreting their NCLEX practice questions accuracy as indicating either more readiness or less readiness than it actually represents — and making preparation decisions based on an inaccurate readiness signal. The accuracy expectation gap is the most common version: candidates who expect their NCLEX practice accuracy to match nursing school examination passing standards (75 to 80 percent) misread 55 to 60 percent practice accuracy on a well-calibrated question bank as significantly below standard when it actually represents at-threshold readiness. These candidates extend preparation unnecessarily, develop anxiety about preparation adequacy that impairs preparation quality, or change to lower-difficulty question banks that produce the 75 percent accuracy they expect — creating an inflated readiness signal that the actual examination then contradicts. The opposite misreading is also common: candidates who achieve 65 to 70 percent practice accuracy on a low-difficulty question bank incorrectly conclude they are well above the readiness threshold and proceed to the examination with genuine preparation gaps that a well-calibrated question bank would have identified.
The Specific Fix
Calibrate your NCLEX practice questions accuracy expectations against the correct readiness threshold: 55 to 60 percent overall accuracy on a well-calibrated question bank with an upward trend across at least three consecutive weeks, no content category below 50 percent, NGN accuracy above 50 percent tracked separately, and a passing-range full simulation within two weeks of the exam date. If your current question bank is producing practice accuracy above 70 percent consistently, the bank’s difficulty may be below NCLEX calibration — complete 25 to 30 NCSBN official sample questions and compare your accuracy to your bank’s accuracy to assess whether the difficulty discrepancy is significant. Track your accuracy trend rather than point-in-time accuracy: a consistent upward trend from 50 percent to 58 percent across six weeks indicates better readiness than a flat 63 percent that has not improved in three weeks, because the trend reflects developing clinical reasoning competency while the flat higher number reflects a ceiling on a potentially low-difficulty bank.
Reason 8: Exam-Day Performance Gap — Anxiety Impairing Clinical Reasoning
The Failure Mechanism
The eighth reason students fail the NCLEX is the exam-day performance gap — the difference between NCLEX practice questions accuracy that meets or approaches the readiness threshold and the actual examination performance that falls below the passing standard. This gap is produced by the anxiety response that exam-day conditions trigger: the testing center environment, the stakes of the examination, the unfamiliar physical conditions, and the CAT algorithm’s adaptive difficulty all activate a threat response that elevates cortisol, narrows attention, and degrades the prefrontal cortex regulatory capacity that systematic clinical reasoning requires. A candidate whose practice accuracy has been consistently 58 to 62 percent may discover that their exam-day reasoning quality is measurably lower — not because their clinical knowledge has changed but because the anxiety-impaired cognitive state that the exam’s conditions produce is accessing that knowledge less efficiently than the calm home practice environment did.
The Specific Fix
Address the exam-day performance gap through two parallel preparation tracks. First, simulate testing center conditions during weekly full-length NCLEX practice questions simulations: sit at a desk (not a couch), remove all personal devices from the workspace, set room temperature slightly cooler than comfortable, use only a visible timer for pacing, and apply the interquestion reset (one slow breath, hands flat, brief eyes closed) after every question throughout the session. This environmental and behavioral simulation conditions the clinical reasoning process to the testing center’s physical demands so that those conditions are familiar preparation constraints on exam day rather than novel stressors. Second, practice the three in-exam performance anchors until they are conditioned responses rather than deliberate techniques: the interquestion reset after every question, the difficulty reframe (this question is hard, which means the algorithm is tracking strong performance — apply my framework and move forward), and the process-focus mantra (this question, this reasoning, now). These anchors, conditioned through six weeks of NCLEX practice questions sessions, fire automatically on exam day and interrupt the anxiety spiral before it degrades clinical reasoning quality.
The Common Thread: Effort Misaligned With What the Exam Measures
Across all eight failure reasons, the common thread is preparation effort misaligned with what the NCLEX examination actually measures. The examination measures clinical judgment — the ability to apply specific clinical reasoning frameworks to specific patient clinical scenarios to identify the correct nursing priority action. Every failure reason in this guide describes a specific way that high preparation effort can be invested in activities that feel like clinical judgment development but produce something other than it: content familiarity from answer-checking, content review from misdiagnosed reasoning errors, question volume from untimed sessions that build the wrong temporal calibration, traditional pattern recognition from deferred NGN practice, inflated readiness signals from low-difficulty question banks, depleted cognitive capacity from preparation without recovery, anxiety-driven decisions from accuracy expectation mismatches, and clinical reasoning degradation from an anxiety response that preparation never trained against.
The candidates who pass the NCLEX on their first attempt are not those who avoided all of these failure patterns naturally. They are those who applied preparation behaviors aligned with what the examination actually measures — full rationale protocol that builds clinical reasoning rather than content familiarity, error type classification that identifies the correct intervention rather than defaulting to content review, timed practice that calibrates clinical reasoning to the examination’s temporal constraints, NGN format integration that develops the specific cognitive skills the current examination tests, quality question bank selection that produces accurate readiness signals, recovery protection that maintains cognitive capacity for the full preparation period, accurate readiness assessment that makes data-based exam decisions, and exam-day preparation that conditions clinical reasoning to perform under testing center conditions. These are learnable, practicable, completely within reach behaviors. They are the preparation that passes.
- How to self-diagnose which failure reason applies to you: Review your last two weeks of NCLEX practice questions sessions and ask: am I completing the full four-question rationale protocol on every question? Am I classifying every incorrect answer by error type rather than defaulting to content review? Am I practicing under 90-second timed conditions with milestone checks? Am I including 30 to 35 percent NGN format content daily and tracking NGN accuracy separately? Is my question bank producing accuracy in the 55 to 65 percent range? Do I have two designated rest days per week? Am I interpreting my accuracy against the 55 to 60 percent threshold rather than nursing school standards? Am I simulating testing center conditions in weekly full-length sessions? Any ‘no’ answer identifies the specific failure pattern most likely contributing to preparation inefficiency.
- The fastest single preparation change for most struggling candidates: Apply the complete four-question rationale protocol to every NCLEX practice question in tomorrow’s session — not just incorrect answers, every question. This single change, applied consistently across two weeks, produces more measurable accuracy improvement than any other single preparation behavior change because it converts every practice question from a correct-answer confirmation event into a clinical reasoning development event. Most candidates who implement this change report that the rationale review feels more demanding and more time-consuming than their previous approach — which is exactly the signal that it is producing the clinical reasoning development that answer-checking was not.
- What to do if you have already failed once: The Candidate Performance Report issued after a not-passing result is the most specific preparation intelligence available for your second attempt — more accurate than any diagnostic assessment because it reflects actual exam performance at actual difficulty under actual exam conditions. Read the CPR to identify which content categories were below the passing standard. For each below-standard category, classify the gap type (knowledge gap, reasoning pattern error, NGN format performance gap, or approach methodology failure under exam conditions) before designing any preparation intervention. Make structural changes to your preparation approach for each identified gap type rather than repeating the first approach with more intensity. The second attempt most often fails for the same reason as the first when the structural preparation changes are not made.
Conclusion
The most common reasons students fail the NCLEX are not inadequate effort, insufficient intelligence, or poor clinical aptitude. They are specific, identifiable preparation behavior misalignments that direct high-effort preparation away from the clinical reasoning competency the examination measures toward preparation activities that produce the subjective experience of productivity without the clinical judgment development that exam performance requires. Answer-checking instead of analytical rationale review. Misdiagnosing reasoning errors as content gaps. Untimed practice sessions. Deferred NGN format preparation. Low-quality or outdated question banks. Preparation without recovery. Accuracy expectation mismatches. Exam-day performance gaps from unconditioned anxiety responses.
Each of these failure patterns is addressable with a specific, concrete preparation behavior change that does not require additional resources, additional hours, or exceptional effort beyond what most candidates are already investing. It requires redirecting existing effort toward preparation behaviors aligned with what the examination actually measures. Apply the full rationale protocol to every NCLEX practice question. Classify every incorrect answer by error type. Practice under timed conditions from day one. Integrate NGN format from day one. Verify your question bank is well-calibrated. Protect your cognitive recovery. Calibrate your accuracy expectations correctly. And condition your clinical reasoning to perform under testing center conditions. These eight changes, applied together, address the eight most common reasons students fail — and position the preparation for the first-attempt passing result that the examination is designed to confirm.