Every nursing candidate who has sat down with a practice question bank and read the rationale for an incorrect answer has had a version of the same experience: the rationale makes complete sense after the fact, but something about the way the question was constructed prevented the correct reasoning from emerging during the question itself. The clinical knowledge was present. The correct answer was in the option set. The rationale, when read, was immediately comprehensible. But the question still produced the wrong answer — and the candidate cannot fully articulate why.
This experience is not a knowledge failure. It is a question-reading failure — a mismatch between what NCLEX questions are actually looking for and what the candidate’s question-engagement approach is designed to find. Every NCLEX question in 2026, regardless of its format, is engineered to test a specific cognitive competency in a specific way — and understanding the engineering behind the question, rather than only the clinical content within it, is what allows candidates to approach every question from the correct cognitive stance before any clinical reasoning begins.
This guide takes the question-anatomy perspective that most preparation guidance does not: dissecting what NCLEX questions are actually built to test at the structural level, what the question’s design reveals about which cognitive approach will produce the correct answer, what distractor options are specifically engineered to attract and why they work on candidates who have not understood the question’s design, and how this structural understanding changes the approach to every question type in every clinical content area. The goal is not to teach question tricks — the NCLEX questions resist tricks by design. The goal is to understand what the examination is genuinely looking for so that preparation develops the competency it measures rather than strategies that mimic it.
What NCLEX Questions Are Actually Measuring
The foundational misunderstanding about NCLEX questions is that they are primarily testing whether candidates know clinical content. They are not. They are testing whether candidates can use clinical content within a specific reasoning framework to make the correct clinical decision for a specific patient at a specific clinical moment.
The Distinction Between Content Knowledge and Clinical Reasoning
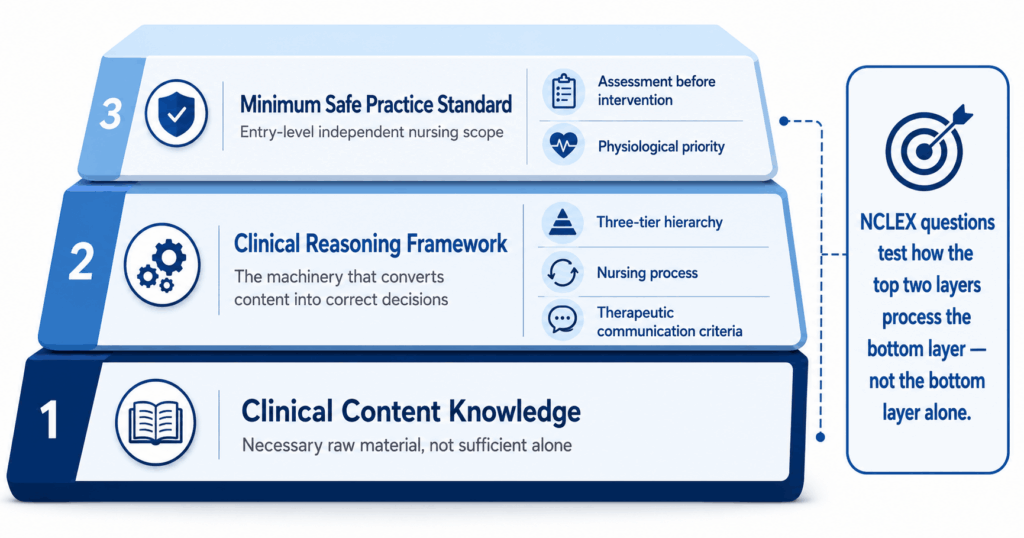
Clinical content knowledge is necessary but not sufficient for NCLEX questions. A candidate must know that furosemide is a loop diuretic that causes potassium loss and monitoring of potassium levels is essential. But the NCLEX question tests what the nurse does when a patient on furosemide presents with muscle weakness, cramping, and an irregular heart rate — which requires not just knowing the drug’s side effects but applying the nursing priority framework to a specific clinical constellation to determine that hypokalemia is the most urgent hypothesis, that the immediate priority is assessment of serum potassium and cardiac rhythm, and that the action threshold for potassium below 3.5 mEq/L includes provider notification before the next dose. The clinical content is the raw material. The clinical reasoning is the machinery that converts the raw material into the correct answer. NCLEX questions test the machinery, not just the material.
The Minimum Safe Practice Standard
Every NCLEX question is written against a specific standard: what would a minimally competent entry-level registered nurse do in this clinical situation? This standard is important because it defines the correct answer as the action a beginning-level nurse would take — not the action a highly experienced specialist nurse might take, not the action a physician would take, and not the most comprehensive theoretically ideal nursing response. NCLEX questions consistently select correct answers that reflect the independent nursing scope of practice rather than delegated medical actions, the assessment-before-intervention sequence rather than immediate treatment initiation, and the physiological priority hierarchy rather than patient preference or convenience. Candidates who answer NCLEX questions from the perspective of a highly experienced nurse, a physician, or a patient-preference-first framework will consistently select plausible but incorrect options that reflect a different clinical standard than the one the question is built around.
The Transferable Framework Requirement
The most important structural feature of NCLEX questions in 2026 is that they are consistently written to test transferable framework application rather than specific scenario familiarity. The cardiovascular NCLEX question that tests ABC priority framework application is testing the same cognitive competency as the respiratory question, the neurological question, and the obstetric question that test the same framework in different clinical contexts. A candidate who has internalized the framework will transfer it correctly to every novel scenario the question presents. A candidate who has memorized correct answers to specific cardiovascular scenarios will answer that scenario correctly and fail when the same framework appears in a different clinical context they have not specifically practiced. This is why NCLEX question writers deliberately construct scenarios in unfamiliar clinical combinations — the combination is novel; the framework is always the same.
The Anatomy of a Traditional NCLEX Question

Every traditional multiple choice NCLEX question has a specific anatomy — structural components that each serve a defined function in the question’s construction and that, when understood, reveal what the question is testing before any clinical reasoning begins.
The Stem: What the Question Is Actually Asking
The question stem of a traditional NCLEX question contains two distinct layers that must be identified separately before engaging any answer option. The clinical context layer provides the patient information that establishes the scenario: patient demographics, diagnosis or presenting situation, relevant history, current vital signs or assessment findings, and any clinical context that makes some options correct and others incorrect for this specific patient. The question layer specifies what clinical decision is being requested: what does the nurse do first, what assessment takes priority, what patient teaching is most important, what response is most therapeutic. The most important habit for approaching NCLEX questions is reading the question layer first — before any detailed engagement with the clinical context — to establish what cognitive process the question requires. A candidate who identifies that the question asks for the priority assessment activates the physiological hierarchy before reading the options. A candidate who reads the clinical context first and then the question layer has already formed clinical associations that may compete with the framework application the question requires.
The Correct Option: What It Must Demonstrate
The correct option in a traditional NCLEX question is always the option that most accurately reflects the nursing action a minimally competent entry-level nurse would take given the clinical context and the clinical question asked. The correct option is not necessarily the most comprehensive nursing response, the most advanced clinical intervention, or the most impressive demonstration of nursing expertise. It is the option that correctly applies the relevant clinical reasoning framework — the ABC hierarchy, the nursing process sequence, the therapeutic communication technique criteria — to the specific patient context provided in the stem. NCLEX questions are specifically designed so that the correct option cannot be identified from general nursing knowledge alone — the clinical context in the stem provides the specific patient details that make the framework application produce the correct priority rather than a different priority that would be correct for a different patient. Candidates who identify the correct answer without engaging the specific stem context may be correct on familiar scenarios and systematically wrong on unfamiliar ones.
The Distractor Engineering
The distractor options in NCLEX questions are not randomly selected incorrect answers. They are precisely engineered to attract candidates who have specific, predictable reasoning gaps — and understanding the distractor engineering reveals what reasoning error each option is designed to identify. The most common distractor types in NCLEX questions: the almost-correct distractor (an option that is a correct nursing action in general but is not the highest priority for this specific patient at this specific clinical moment — this distractor attracts candidates who recognize the option as clinically correct without applying the priority hierarchy to the specific scenario), the nursing-school-rewarded distractor (an option that would be taught as a standard nursing intervention in a content review but that requires physician collaboration, delegation, or goes beyond independent nursing scope for the specific situation — this distractor attracts candidates who are answering from content familiarity rather than from the minimum safe practice standard), and the psychosocial-before-physiological distractor (a communication or emotional support option presented in a scenario where unaddressed physiological needs take priority — this distractor attracts candidates whose priority framework application does not consistently apply the physiological-before-psychosocial sequence).
The Anatomy of NGN NCLEX Questions
NGN NCLEX questions have a more complex anatomy than traditional questions because they measure multiple cognitive skills across multiple question formats — each with specific structural features that reveal what they are testing and how to approach them correctly.
The Unfolding Case Study: A Living Clinical Narrative
The anatomy of an unfolding case study set of NGN NCLEX questions is fundamentally different from any traditional question structure: it is a living clinical narrative with six evaluation points rather than a static scenario with four options. The opening scenario functions as a patient introduction rather than a question stem — it establishes the baseline clinical picture (patient demographics, presenting situation, initial assessment findings, relevant history) that all six subsequent questions will reference and build on. Each of the six questions then probes a different CJMM cognitive skill at a different point in the patient’s clinical trajectory. The anatomy of each individual question within the set must be read in two layers: the accumulated clinical narrative from all previous questions (what has been established about this patient’s developing situation) and the current question’s specific CJMM skill request (what cognitive operation is being applied to that accumulated narrative at this moment). The most common structural error candidates make with unfolding NGN NCLEX questions is reading each question as a standalone scenario rather than as an evaluation point within a living clinical narrative — which produces answers that are clinically plausible in isolation but incorrect relative to the specific clinical trajectory the narrative has established.
The Bow Tie: Reasoning Made Visible
The bow tie NGN NCLEX question makes the clinical reasoning process structurally visible rather than embedded within option selection. The center node of the bow tie represents the clinical hypothesis the nurse has prioritized — the most urgent explanation for the patient’s current clinical picture. The left-side nodes represent the nursing actions appropriate for that prioritized hypothesis. The right-side nodes represent the assessment parameters the nurse would monitor to evaluate whether the hypothesis is correct and whether the actions are producing the intended outcomes. The anatomical key to bow tie NGN NCLEX questions is that the center selection governs all other selections: a correctly identified center hypothesis produces correct left-side actions and right-side monitoring parameters, while an incorrectly identified center hypothesis makes the correctly identified actions and monitoring incorrect relative to the actual clinical priority. Approach bow tie questions by applying the prioritize hypotheses cognitive skill to the center before engaging either side — the center is not a contextual label but the pivotal clinical judgment the entire question is built around.
Extended Multiple Response: Options as Independent Clinical Decisions
The anatomy of extended multiple response NGN NCLEX questions differs from traditional select-all-that-apply questions in one critical structural feature: there is no defined number of correct options, and the scoring system awards partial credit for each correct selection and reduces credit for each incorrect selection. This structure means each option must be evaluated as an independent clinical decision — does this specific option meet the clinical criteria the question specifies for this specific patient at this specific clinical moment? — rather than as a comparative selection from a defined set. The distractor engineering in extended multiple response NGN NCLEX questions is specifically designed around two failure modes: over-inclusion (selecting options that are generally appropriate nursing actions but are not specifically indicated for this patient’s situation, reflecting familiarity-based selection rather than criteria-based selection) and under-inclusion (failing to select an option that meets the criteria because it is less obvious than the most apparent correct options). The anatomical approach that prevents both failure modes is evaluating each option against a consistent, explicit clinical question: is this option clearly indicated for this specific patient given the specific clinical question being asked?
What the Exam Looks for in Every Clinical Context
Across all NCLEX questions regardless of content area or format, six consistent features distinguish what the examination is looking for from what candidates most commonly provide in their answers.
Patient-Specificity Over General Nursing Knowledge
The most consistent feature of what NCLEX questions look for — across traditional and NGN formats, across all clinical content areas — is patient-specific clinical reasoning rather than general nursing knowledge application. Every NCLEX question provides specific patient context that makes one option more correct than others that would be correct for different patients in similar but not identical situations. The 68-year-old patient with COPD who presents with confusion, increasing respiratory effort, and SpO2 of 88 percent requires a different assessment priority than the 25-year-old patient with asthma who presents with the same SpO2 — because the COPD patient’s chronic CO2 retention status changes the oxygen administration priority and the acceptable SpO2 target in ways that the asthma patient’s history does not. NCLEX questions consistently reward candidates who extract and apply the specific patient context the stem provides rather than candidates who apply the correct nursing knowledge for the most common patient with this clinical presentation.
Assessment Before Action — With Specific Exceptions
NCLEX questions consistently look for the assessment-before-intervention sequence when the question asks what the nurse does first in a non-emergency clinical scenario — but this principle has specific, consistently tested exceptions that candidates who apply it too broadly will miss. The exceptions: when the question stem establishes that the relevant assessment has already been completed (a previously documented finding, a reported symptom that is already documented, a vital sign already recorded in the stem), the correct first action shifts from assessment to intervention because the assessment data is already available. When the scenario presents an immediately life-threatening situation — cardiac arrest, airway obstruction, active hemorrhage — the correct response bypasses the nursing process assessment step because delay for additional assessment in these situations constitutes clinical negligence rather than safe practice. When a previously ordered intervention is due and the clinical context does not suggest contraindication, administering the intervention may be correct before the additional assessment that context does not require. NCLEX questions are specifically designed with these exceptions to identify candidates who apply the assessment-before-action principle mechanically rather than clinically.
The Physiological Urgency Signal
The feature that NCLEX questions most reliably use to establish the correct priority answer is the physiological urgency signal — the specific clinical data point in the stem that indicates an unaddressed physiological threat requiring immediate nursing attention. In priority questions, the correct option almost always corresponds to the option that addresses the physiological urgency signal most directly and most immediately. The challenge in reading NCLEX questions is that the physiological urgency signal is rarely the most obviously presented data point — it is often embedded within a complex clinical scenario alongside multiple psychosocial signals, patient preferences, family concerns, and less urgent physiological findings, any of which could attract attention from a candidate who is reading the stem broadly rather than scanning specifically for ABC threats and unaddressed physiological needs. The question-reading habit that most directly improves priority question accuracy is the deliberate physiological urgency scan — reading the stem with the specific goal of identifying the highest-tier physiological signal before engaging any other clinical information.
The Nursing Scope Boundary
NCLEX questions look for nursing actions within the independent nursing scope of practice for the clinical context presented — and they consistently include distractor options that represent actions beyond that scope, require physician orders the question has not established exist, involve delegating to personnel who cannot legally perform the action in the presented context, or represent institutional practices rather than independent nursing judgment. The nursing scope boundary is one of the most reliable distractor detection tools available for traditional NCLEX questions: any option that requires a physician to initiate, requires a physician order that is not already established in the stem, or represents an advanced practice action for a staff nurse clinical scenario is almost certainly a distractor regardless of how clinically appropriate the action might be in a real-world context where physician orders are readily available. Identifying this scope boundary before engaging option evaluation significantly narrows the option set to options that are clinically appropriate within the question’s specific constraint.
How Understanding Question Design Changes Your Preparation
The question-anatomy perspective on NCLEX questions has specific, actionable implications for how preparation sessions should be structured — implications that differ meaningfully from the content-coverage approach that most candidates default to.
Rationale Review as Question Deconstruction
When rationale review is understood through the question-anatomy lens, it becomes question deconstruction rather than correct-answer confirmation. For every NCLEX question in every practice session, the post-answer rationale review should produce four specific analytical findings: which clinical reasoning framework the correct option applied and how it applied it to the specific patient context, what each distractor option was specifically engineered to identify (which reasoning gap it targets), what the stem’s physiological urgency signal was and whether it was identified before options were read, and what the question’s specific patient context contributed to making this option correct rather than a different option that would be correct for a different patient. This four-finding deconstruction takes more time than answer-checking but produces more preparation value per question than any other rationale review approach — because it builds the question-reading skill that transfers to every novel scenario rather than the content familiarity that only transfers to similar scenarios.
Building the Question-Reading Pre-Option Sequence
Understanding what NCLEX questions are looking for produces a specific pre-option sequence that should be applied to every question before any answer option is read: first, identify the question layer (what clinical decision is being requested — assessment, intervention, priority action, patient teaching, therapeutic communication), second, apply the relevant clinical reasoning framework for that question type (physiological hierarchy for priority questions, nursing process sequence for process questions, therapeutic communication technique criteria for communication questions), third, scan the clinical context for the physiological urgency signal that the framework should be applied to, fourth, form a preliminary correct answer from the framework application before reading any option. This pre-option sequence — which takes approximately ten seconds — prevents the most common question-reading error: engaging option evaluation before the clinical reasoning framework has been activated, which allows distractor engineering to compete with framework application rather than occurring after it.
Tracking Question Type Errors Separately From Content Errors
The question-anatomy perspective reveals a preparation tracking distinction that content-focused error analysis misses: the difference between a content error (the clinical principle required for the correct answer was not in the accessible knowledge base) and a question-reading error (the clinical principle was available but the question’s design prevented its correct application — the physiological urgency signal was missed, the distractor engineering attracted attention away from the framework application, or the question layer was misidentified). These two error types require different preparation responses. Content errors require content review. Question-reading errors require deliberate practice of the pre-option sequence and the physiological urgency scan — not more clinical content but more deliberate question-reading discipline. Candidates who track these two error types separately consistently discover that a significant proportion of their incorrect NCLEX questions are question-reading errors rather than content errors — and that addressing the question-reading skill directly produces faster accuracy improvement than the equivalent additional content review investment.
- The single most useful pre-exam question-reading drill: Before each practice session, spend five minutes reading five question stems only — no options, no rationale — and for each one, identify the question layer, the relevant clinical framework, and the physiological urgency signal embedded in the stem. Then check the correct option against your pre-option prediction. The accuracy of your prediction before reading any option measures how well your question-reading skill is developing, independent of whether your clinical content knowledge is sufficient to confirm the answer through rationale review.
- How to use distractor engineering as a learning tool: For every incorrect answer you select, spend 60 seconds identifying which distractor type it was — almost-correct but wrong priority for this patient, nursing-school-rewarded but outside independent scope, or psychosocial-before-physiological in a scenario requiring physiological priority. Naming the distractor type converts an incorrect answer from a content gap signal into a question-reading pattern signal — and question-reading pattern signals produce more actionable preparation adjustments than vague awareness that a question was missed.
- What to notice about questions you answer correctly: Questions answered correctly after genuine reasoning are the most reliable indicators of true clinical judgment development. Questions answered correctly through pattern recognition (the scenario looked familiar, the option felt right) are less reliable because they reflect the exact competency that the NCLEX question design is built to test beyond. For correctly answered questions, note whether you activated the relevant framework before reading options or whether you recognized the scenario and selected the correct option through familiarity — the former indicates genuine framework fluency, the latter indicates pattern recognition that may fail on novel presentations of the same framework.
Conclusion
NCLEX questions in 2026 are not primarily knowledge tests dressed in clinical scenarios. They are clinical reasoning tests that use clinical scenarios as the vehicle — and understanding the distinction changes everything about how preparation should develop the competency they measure. The examination is looking for patient-specific framework application rather than general nursing knowledge recall. It is looking for assessment before action with the specific clinical exceptions that distinguish mechanical from clinical application. It is looking for the physiological urgency signal identified before options generate competing clinical associations. It is looking for nursing actions within independent scope rather than actions that require physician initiation or orders not established in the stem.
Every practice session that applies the question-anatomy perspective — identifying the question layer before engaging clinical context, scanning for the physiological urgency signal before reading options, deconstructing distractor engineering rather than only confirming the correct answer, and tracking question-reading errors separately from content errors — is building the specific competency that NCLEX questions measure. That competency is not knowledge. It is the systematic clinical reasoning that uses knowledge as its input and patient safety as its output. That is what the examination is really looking for. And it is exactly what deliberate, anatomy-aware preparation builds.