The NCLEX 2026 preparation landscape is full of advice — from nursing school faculty, from peers who recently passed, from social media nursing communities, from commercial preparation resource providers, and from the enormous ecosystem of nursing student forums where preparation anxiety gets amplified and incomplete information gets shared as fact. Some of that advice is accurate and well-grounded in the current examination’s requirements. A significant portion of it is incomplete, outdated, or reflects the specific preparation context of the advice-giver rather than any generalizable truth about what the examination requires and what preparation behaviors predict passing.
This guide presents the honest truths about the NCLEX 2026 — not the reassuring narratives that preparation resource marketing produces and not the anxiety-amplifying warnings that nursing student forums generate, but the accurate, evidence-grounded, sometimes counterintuitive realities about what the examination measures, what genuinely predicts first-attempt passing, what preparation behaviors feel productive but aren’t, and what every candidate in 2026 needs to understand before investing weeks of effort in a preparation approach that may not be aligned with what the current examination actually tests. Some of these truths will be uncomfortable. Most of them are actionable. All of them are based on what the NCLEX 2026 actually is rather than what candidates wish it were or fear it might be. The truths in this guide are organized as the preparation realities that most candidates encounter as surprises — things they wish someone had told them before they began preparation rather than things they discovered mid-preparation when changing course becomes more costly. Reading this guide before beginning serious NCLEX 2026 preparation is the most efficient use of the time it takes to read it.
Truth 1: More Questions Does Not Equal More Readiness
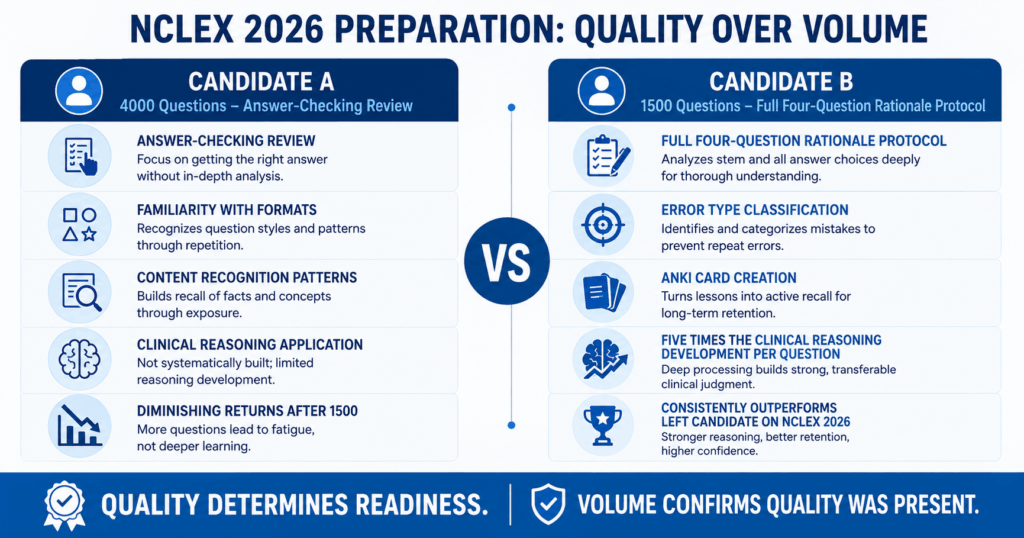
The most pervasive and most preparation-damaging myth in NCLEX 2026 preparation communities is that question volume is the primary determinant of readiness — that completing more practice questions produces more clinical reasoning development and that the candidate who completes 4,000 questions is necessarily better prepared than the candidate who completes 1,500.
What Question Volume Actually Predicts
Question volume predicts readiness only when each question is accompanied by full rationale review quality — and the correlation between volume and readiness collapses entirely when rationale quality is absent. A candidate who completes 4,000 questions with answer-checking review (reading the correct answer’s rationale and moving on) has accumulated familiarity with question formats and content recognition patterns. They have not necessarily developed the clinical reasoning application skill that the NCLEX 2026 CAT algorithm measures — because that skill is built through the rationale analysis that extracts clinical reasoning principles from every option of every question, not from the accumulation of question exposure alone. A candidate who completes 1,500 questions with full four-question rationale protocol applied to every question and error type classification for every incorrect answer has extracted approximately five times the clinical reasoning development per question as the answer-checking candidate. The 1,500-quality-question candidate will consistently outperform the 4,000-answer-checking candidate on the NCLEX 2026 regardless of what the volume difference suggests about preparation investment.
The Diminishing Returns Reality
The honest truth about question volume in NCLEX 2026 preparation is that meaningful returns diminish after approximately 1,500 questions with full rationale quality and essentially disappear after 3,000 questions with the same quality — not because clinical content has been exhausted but because the clinical reasoning patterns that new questions reveal become increasingly redundant with patterns that previous questions have already established. A candidate in week six of preparation who has completed 2,000 questions is encountering clinical scenarios that test the same reasoning frameworks in slightly different presentations rather than revealing genuinely new clinical reasoning territory. At this point, the preparation investment that produces the most additional clinical reasoning development is targeted review of the specific gaps identified by that week’s accuracy data — not more undifferentiated question volume. Continuing to add question volume at this stage produces the subjective experience of preparation productivity without the clinical reasoning development that would justify it.
The Truth About What Volume Metrics Reveal
When a candidate reports completing a high question volume in preparation for NCLEX 2026, the most clinically relevant follow-up question is not how many questions but what was the rationale review quality for each one. A weekly question total of 350 questions with complete four-question rationale protocol, error type classification, and Anki card creation produces more measurable clinical reasoning improvement in the subsequent week’s practice than 700 questions with cursory rationale review — because the 350-quality-question week has built durable, retrievable clinical reasoning that the next session can apply, while the 700-answer-checking week has built transient familiarity that decays rapidly without consolidation. Reframe the preparation quality metric from questions completed per week to clinical reasoning principles consolidated per week — and preparation efficiency will improve regardless of whether question volume increases, decreases, or stays the same.
Truth 2: Feeling Unprepared Before the Exam Is Normal and Not Diagnostic

One of the most universally reported NCLEX 2026 experiences — and one of the most universally misinterpreted — is the subjective feeling of being underprepared that almost every candidate experiences in the days before the examination, regardless of how thoroughly they have actually prepared.
Why Every Candidate Feels Underprepared
The subjective sense of insufficient preparation before the NCLEX 2026 is produced by three systematic distortions that affect nearly every candidate regardless of actual readiness. First, the preparation process reveals gaps continuously — every week of preparation exposes clinical content areas that require additional work, and the candidate who has been preparing for six weeks has a far more specific and detailed awareness of their clinical reasoning gaps than the candidate who began preparation yesterday. This progressive gap awareness creates the impression that preparation is revealing an expanding deficit rather than a narrowing one — even when the trend is precisely the opposite. Second, the NCLEX accuracy expectation gap distorts the subjective readiness assessment: candidates who have been trained to associate 75 to 80 percent accuracy with adequate preparation consistently feel underprepared when their quality question bank shows 57 to 60 percent accuracy — which is actually at or above the readiness threshold for a well-calibrated question bank. Third, exam anxiety generates a threat-state that the prefrontal cortex interprets as evidence of danger — and the brain’s threat-detection system does not reliably distinguish between the genuine danger of being clinically underprepared and the perceived danger of facing an important examination while feeling uncertain. The result is a feeling of inadequacy that is experienced as genuine insight into preparation status but is actually a normal physiological anxiety response.
What Actually Predicts Readiness — Not Feelings
The honest truth about readiness assessment for NCLEX 2026 is that the feeling of readiness is among the least reliable available indicators of actual exam-day performance — because it is systematically distorted in ways that produce both false confidence (candidates who feel ready because they have covered comprehensive content but have not developed clinical reasoning application) and false inadequacy (candidates who feel underprepared despite meeting all four readiness benchmarks because exam anxiety is generating a threat response). The reliable readiness indicators are the four benchmarks that practice analytics produce: overall accuracy above 55 to 60 percent across at least 1,500 completed quality questions with an upward trend, no content category below 50 percent accuracy in the most recent simulation, NGN accuracy above 50 percent tracked separately, and a passing-range full simulation within two weeks of the exam date. Candidates who meet all four benchmarks consistently across three weeks have the data-based go signal regardless of how prepared or unprepared they feel. Candidates who feel ready but whose benchmark data shows persistent below-standard categories have genuine preparation gaps regardless of how confident the subjective experience is. Trust the data. Acknowledge the feeling without letting it make the decision.
The Danger of Feeling-Driven Exam Date Decisions
The feeling of unpreparedness drives two specific NCLEX 2026 decisions that consistently produce worse outcomes than data-based decisions. The first is indefinite exam date extension — continuing to delay the exam past the point where all four readiness benchmarks are met because the feeling of inadequacy persists despite the data showing readiness. This extension produces additional preparation time that accumulates Anki reviews, runs more practice sessions, and deepens anxiety without producing meaningful additional clinical reasoning development — because the benchmarks have already confirmed that the clinical reasoning competency the exam measures has been built. The second is panic-driven preparation change — abandoning a systematic preparation approach that is producing benchmark improvement because the feeling of inadequacy makes it feel insufficient, and switching to a different resource, a different strategy, or an intensive cramming approach that disrupts the consolidation process the systematic approach was building. Both decisions are produced by treating feeling as evidence. The honest NCLEX 2026 truth is that feeling-driven exam decisions are almost always worse than benchmark-data-driven decisions.
Truth 3: The Exam Length Tells You Nothing About Your Result
Among all the NCLEX 2026 anxieties that candidates carry into the testing center, the anxiety about exam length — how many questions they will receive and what that number means about their performance — is both the most common and the most based on misunderstanding of how the CAT algorithm works.
The 75-Question Myth
The persistent myth in NCLEX 2026 candidate communities is that an exam ending at 75 questions means the candidate passed — that the minimum question count is a positive signal. This belief is incorrect. The exam ends at 75 questions when the CAT algorithm reaches 95 percent statistical confidence that the candidate’s ability estimate is either clearly above or clearly below the passing standard — both outcomes can produce a 75-question exam. A candidate whose ability estimate is well above the passing standard after 75 questions receives a passing result. A candidate whose ability estimate is well below the passing standard after 75 questions receives a not-passing result. Both are 75-question exams. The question count at the minimum boundary indicates high statistical confidence in the determination — it does not indicate the direction of the determination. Candidates who exit at 75 questions and feel certain they passed because of the length, and candidates who exit at 75 questions and feel certain they failed because the exam felt hard — both are drawing conclusions from information that contains no result signal.
The 150-Question Myth
The opposite myth — that an exam running to 150 questions means the candidate failed or is barely passing — is equally inaccurate for NCLEX 2026. The exam reaches 150 questions when the candidate’s ability estimate has remained near the passing standard boundary long enough that the maximum item count was reached before 95 percent confidence was achieved. This means the candidate’s performance kept the algorithm uncertain about whether their ability was above or below the standard — which can happen when a candidate is performing strongly but with enough variability that the estimate oscillates near the threshold. A candidate who receives 150 questions and passes has simply provided a response pattern that took more questions for the algorithm to classify with confidence. The commonly expressed belief that a 150-question exam indicates the candidate barely squeaked through reflects a fundamental misunderstanding of how the CAT algorithm works. The exam length is a measurement efficiency data point — it reflects how quickly the algorithm gathered sufficient evidence, not how high or low the ability estimate landed.
What to Do With Exam Length Information
The honest NCLEX 2026 truth about exam length is that the optimal response to any question count is complete indifference during the examination and complete indifference after it. During the examination, knowing the question count is useful only for pacing — confirming at milestone checkpoints that the session is on pace for the five-hour time allocation. It is not useful for performance assessment, result prediction, or anything else that candidates typically use it for. After the examination, the question count provides no reliable information about the result — and engaging with post-exam question-count speculation in nursing student communities before official results are available produces anxiety without insight. The only productive post-exam activity while awaiting NCLEX 2026 results is giving the nervous system the recovery it deserves after a demanding clinical reasoning performance. Everything else is noise.
Truth 4: The NGN Is Not Optional Preparation — It Is the Exam
Among the NCLEX 2026 preparation truths that candidates most need to hear before beginning preparation, the most consequential for candidates who have relied on pre-2023 preparation advice is this: the NGN clinical judgment formats are not an add-on to the NCLEX — they are a core component of the examination whose proportion has increased with the April 2026 test plan update, and preparation that does not address them specifically is preparation for a version of the examination that no longer exists.
Why NGN Preparation Keeps Getting Deferred
The honest assessment of why so many NCLEX 2026 candidates defer NGN-specific preparation until the final weeks is that NGN format questions are harder, less familiar, and more cognitively demanding than traditional multiple choice questions — and preparation systems naturally drift toward the activities that feel most productive, which are the ones most similar to the familiar nursing school examination format. Traditional multiple choice sessions produce recognizable accuracy metrics, rationale feedback, and the satisfying efficiency of completing 50 questions in 75 minutes. NGN unfolding case study sets produce confusion about format mechanics, unfamiliar question structures, partial credit responses that feel ambiguous, and the unsatisfying experience of six questions taking 10 minutes rather than one question taking 90 seconds. The natural preparation response to this discomfort is to do more traditional questions and return to NGN format later — which produces exactly the preparation gap that the NCLEX 2026’s higher NGN proportion penalizes most directly.
What NGN Underpreparation Actually Costs
The cost of NGN underpreparation in NCLEX 2026 is not a penalty applied to a separate NGN section — it is a systematic reduction in the ability estimate that the CAT algorithm builds from the full response pattern, because NGN items contribute to the ability estimate at every point in the session where the algorithm selects them. A candidate whose traditional format accuracy is 65 percent and whose NGN accuracy is 41 percent is providing an ability estimate that reflects a blended performance significantly below what the traditional accuracy alone would predict. With the April 2026 NGN proportion increase, this blended effect is larger than it was in 2023 or 2024 — more NGN items per session means more below-standard ability evidence per session for the underprepared candidate. The practical preparation implication is direct: begin NGN format practice in the first week of NCLEX 2026 preparation, integrate it at 30 to 35 percent of daily questions throughout the preparation period, track NGN accuracy separately from overall accuracy in every weekly micro-audit, and treat NGN accuracy below 50 percent as a readiness gap requiring specific intervention — not as an acceptable concession to format unfamiliarity.
The CJMM Action Verb Is the NGN Key
The single most important NGN preparation insight for NCLEX 2026 candidates who are overwhelmed by the format complexity is that every NGN question communicates its required cognitive skill through the action verb in the question stem — and identifying that action verb before reading any answer option eliminates the most common and most costly NGN error of applying the wrong cognitive process to the question. Identify or select = recognize cues skill. Interpret or explain what this indicates = analyze cues skill. Prioritize or rank by urgency = prioritize hypotheses skill. Generate or identify nursing actions = generate solutions skill. Implement or initiate = take action skill. Determine effectiveness or select findings indicating improvement = evaluate outcomes skill. This action verb identification takes three to five seconds per question and directs the clinical reasoning approach before distractors create competing clinical associations. NCLEX 2026 candidates who build this action verb habit across six weeks of NGN practice will find it fires automatically on exam day — which is the preparation outcome the habit-building investment is designed to produce.
Truth 5: Passing Has Nothing to Do With Being the Smartest Nurse
The most psychologically important NCLEX 2026 truth — particularly for candidates who have failed a previous attempt, who are managing performance anxiety, or who are comparing themselves to peers who passed — is that NCLEX passing is not a measure of nursing intelligence, clinical potential, or professional fitness. It is a measure of whether a specific preparation approach developed the specific clinical reasoning competency that the examination measures to a level above the passing standard.
What the NCLEX Actually Measures
The NCLEX 2026 measures clinical judgment — the ability to apply specific clinical reasoning frameworks to clinical scenarios under adaptive difficulty conditions. It does not measure clinical intuition, bedside manner, the ability to think quickly under real patient pressure, communication skills with actual patients, technical clinical skills, or the qualities that make a nurse excellent rather than merely competent at entry level. A candidate who is genuinely talented at all of these qualities but who has not developed the specific CJMM-organized clinical reasoning that the examination tests may score below the passing standard on their first attempt. A candidate who has less natural clinical intuition but who has developed systematic clinical reasoning framework application through deliberate preparation may score well above the passing standard. The NCLEX is a measurement instrument for a specific competency — and the preparation that builds that competency is what determines the result, not the candidate’s broader nursing potential.
What a Failed Attempt Actually Proves
A not-passing NCLEX 2026 result proves one specific thing: the response pattern the candidate produced on that examination did not place their clinical reasoning ability estimate above the passing standard with 95 percent statistical confidence on that occasion. It does not prove that the candidate is not intelligent enough to be a nurse. It does not prove that nursing is the wrong career. It does not prove that the previous preparation approach was fundamentally wrong. It proves that the specific clinical reasoning competency the examination measures was not yet developed to the passing standard level — which is a specific, addressable, time-bounded gap rather than a fixed inadequacy. The nurses practicing today who passed on their second or third attempt are not less capable than those who passed on their first. They are nurses who needed more time or a different preparation approach to develop the specific competency the examination measures — and who developed it. The result is the same license, the same scope of practice, and the same patients.
The Comparison Trap
The nursing student community produces an environment in which NCLEX 2026 performance comparison is both constant and harmful — peers discussing their question counts, their accuracy percentages, their preparation timelines, and their exam experiences in ways that generate social comparison anxiety that impairs both preparation quality and exam-day performance. The honest truth about peer comparison in NCLEX 2026 preparation is that every candidate’s preparation profile is unique — different content gaps, different reasoning pattern errors, different NGN format familiarity, different preparation time constraints, different burnout thresholds, and different exam-day anxiety responses — and no peer’s preparation experience, timeline, or exam outcome is a reliable reference point for any other individual’s preparation or likely outcome. The candidate who needs 10 weeks of preparation is not less capable than the candidate who needs six weeks. The candidate who sits the exam at 150 questions is not performing worse than the candidate who sits at 75. The candidate who is on their second attempt is not less worthy of nursing licensure than the candidate on their first. These comparisons produce anxiety and shame rather than preparation insight — and the most protective preparation decision is deliberate disengagement from comparison-generating information.
- The truth about study groups for NCLEX 2026: Study groups are beneficial when they produce clinical reasoning discussion, mutual accountability, and emotional support that improves individual preparation quality. They are harmful when they become comparison environments where accuracy percentages, question counts, and preparation timelines are shared in ways that generate anxiety rather than insight. A study group where members say I got this cardiovascular question wrong because I applied the physiological hierarchy incorrectly — let us work through the clinical reasoning is an asset. A study group where members say I have completed 2,400 questions this week and my accuracy is 63 percent while someone else has completed 1,800 and scored 58 percent generates social comparison that serves neither candidate.
- The truth about the Quick Results service: The Quick Results service available through Pearson VUE approximately two business days after the NCLEX 2026 for a small fee provides an unofficial pass or fail indication. It is accurate in the overwhelming majority of cases. The truth about what to do with Quick Results before receiving them is this: do not access them unless you are emotionally prepared for either outcome. The Pearson VUE website Quick Results are not confirmed official results — they are an early indication that is almost always accurate. If accessing them will produce several more days of anxiety whether the result is positive or negative, waiting for the state board license verification is the more psychologically sound choice.
- The truth about what happens if you fail: A not-passing NCLEX 2026 result is a preparation data point, not a professional verdict. The Candidate Performance Report that follows a not-passing result is the most specific preparation intelligence available for the second attempt — more precise than any diagnostic assessment because it reflects actual exam performance at actual difficulty under actual exam conditions. Three days of emotional processing followed by CPR analysis and structural preparation change produces a meaningfully different second attempt than the intensity-only approach most candidates instinctively turn to. The second-attempt pass rate for candidates who make structural preparation changes based on CPR analysis approaches the first-attempt pass rate for comparably prepared candidates.
Conclusion: What Is Actually True About Passing the NCLEX in 2026
The NCLEX 2026 passes candidates whose response pattern places their clinical reasoning ability estimate above the passing standard with 95 percent statistical confidence — nothing more and nothing less. It does not pass the candidates who studied the most hours, completed the most questions, felt the most prepared, had the highest nursing school GPA, or received the most encouragement from peers. It passes candidates whose preparation built the specific clinical reasoning competency the examination measures — clinical judgment applied systematically to clinical scenarios through a framework that can be learned, practiced, and confirmed through objective benchmark tracking.
The truths in this guide are not intended to discourage — they are intended to redirect preparation effort toward what actually produces the competency the examination measures. Quality rationale review over question volume. Benchmark data over preparation feelings. Process indifference over exam length monitoring. NGN format integration from day one over deferral to the final weeks. Personal preparation data over peer comparison. And for candidates who have experienced a not-passing result: structural change over intensity repetition, CPR analysis over general additional studying, and three days of honest emotional acknowledgment over immediate return to the approach that produced the first outcome. These truths, applied consistently, are the preparation framework that NCLEX 2026 passing is built on.