NCLEX burnout is not laziness, weakness, or a sign that nursing is the wrong career. It is a predictable physiological and psychological response to sustained cognitive and emotional demand without adequate recovery — and it is far more common among nursing candidates than the preparation advice ecosystem acknowledges. Most NCLEX preparation guidance assumes a candidate who is cognitively fresh, emotionally available, and consistently motivated across a six to twelve week intensive preparation period. It does not account for the candidate who has been working toward this exam through the final grueling semester of nursing school, who graduated into immediate family obligations, who is working part-time while preparing, or who has already sat the exam once and is preparing for a second attempt while managing the psychological weight of a failed result.
NCLEX burnout does not arrive suddenly — it accumulates through weeks of declining preparation quality that the candidate often fails to recognize because the behavioral signs look like preparation problems rather than recovery problems. Declining practice question accuracy is attributed to content gaps that need more study rather than to cognitive fatigue that needs rest. Increasing difficulty concentrating is interpreted as distraction that needs discipline rather than as a physiological signal that the nervous system needs recovery. The emotional flatness that characterizes burnout — the loss of motivation, the sense that the exam will never end, the inability to feel encouraged by progress — is treated as a character problem rather than a clinical state that responds to specific recovery interventions.
This guide addresses NCLEX burnout directly: what it is at a physiological and psychological level, how to recognize it accurately from early warning signs before it becomes preparation-disabling, why the instinctive responses to burnout make it worse rather than better, the specific recovery interventions that address burnout at its physiological root rather than its behavioral surface, how to restructure the preparation approach to prevent recurrence, and when NCLEX burnout signals that something beyond preparation strategy needs attention.
What NCLEX Burnout Actually Is — and What It Isn’t
Accurate understanding of what NCLEX burnout is — and what it is not — is the prerequisite for responding to it correctly rather than making it worse with misidentified interventions.
The Physiological Reality of Burnout
NCLEX burnout is a state of chronic physiological and psychological depletion produced by sustained demand that exceeds the candidate’s recovery capacity. At the physiological level, burnout involves dysregulation of the hypothalamic-pituitary-adrenal axis — the stress response system — producing either chronically elevated cortisol from sustained activation or, paradoxically, blunted cortisol response from HPA axis exhaustion in longer-duration burnout states. Both states impair cognitive function in measurable ways: elevated cortisol reduces hippocampal function and therefore the consolidation of new memories, while blunted cortisol produces the flattened affect, reduced motivation, and cognitive slowing that characterizes advanced burnout. The cognitive impairments that result — reduced working memory, impaired attention, slower information processing, and difficulty with complex problem-solving — are exactly the capacities that NCLEX clinical reasoning requires. A candidate in NCLEX burnout is attempting to build clinical reasoning competency with a nervous system whose primary cognitive capacities are physiologically compromised. More study in this state does not produce more learning; it deepens the depletion.
Burnout vs. Fatigue vs. Laziness
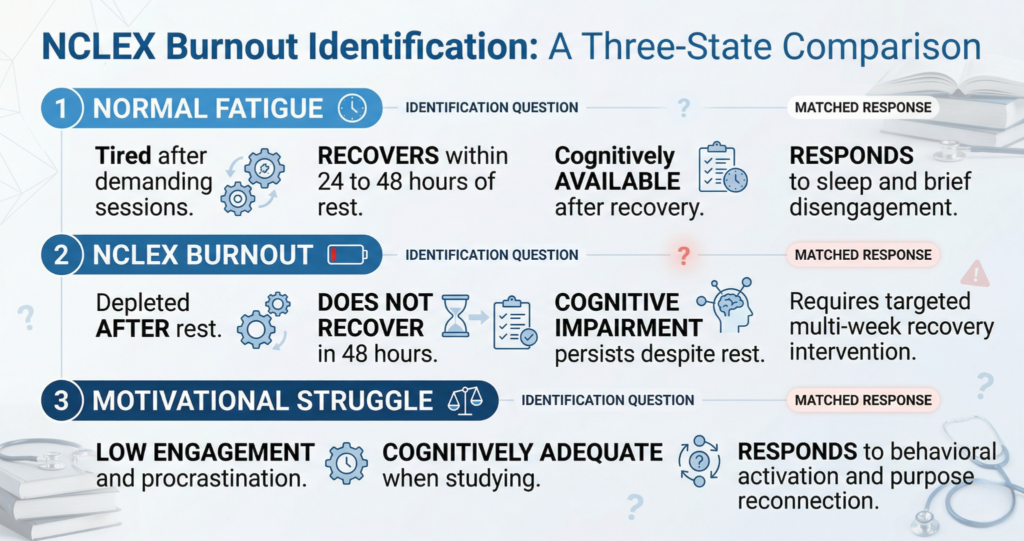
Distinguishing NCLEX burnout from normal preparation fatigue and from motivational struggles is essential because each requires a different response. Normal preparation fatigue is the expected tiredness that follows an intensive study session or a demanding week — it responds within 24 to 48 hours to rest, sleep, and brief disengagement from preparation activity. Burnout does not respond to 24 to 48 hours of rest. A candidate who takes a weekend off from NCLEX preparation and returns on Monday feeling exactly as depleted as they did on Friday has burnout, not fatigue. Motivational struggles — periods of low engagement, procrastination, difficulty beginning study sessions — can accompany burnout but are not equivalent to it and have different causes. A candidate who is not motivated to study but feels physically and cognitively adequate when they do is experiencing a motivational challenge, not NCLEX burnout. A candidate who begins a study session with adequate motivation but finds that they cannot concentrate, retain information, or engage clinically after 20 minutes despite genuine effort is experiencing burnout’s cognitive signature.
Why NCLEX Burnout Is Not a Character Failure
The nursing professional culture’s emphasis on resilience, self-sacrifice, and sustained performance under demanding conditions produces a specific context in which NCLEX burnout is particularly likely to be interpreted as a character failure — an inadequate commitment to the profession, insufficient discipline, or inability to handle the demands that nursing requires. This interpretation is clinically inaccurate and practically harmful. Burnout is not produced by insufficient commitment; it is produced by insufficient recovery relative to the demands placed on the system. The candidates most vulnerable to NCLEX burnout are frequently those with the highest commitment — who study the longest hours, take the fewest breaks, and push through warning signs rather than responding to them because resting feels like abandoning the preparation they are so committed to completing. Responding to NCLEX burnout requires treating it as a physiological state requiring specific recovery interventions rather than as a motivational deficit requiring more discipline. More discipline in a depleted nervous system is not more productive — it is more depleting.
Early Warning Signs of NCLEX Burnout

NCLEX burnout produces recognizable early warning signs that appear weeks before the condition becomes preparation-disabling — and recognizing them at this early stage allows recovery interventions to be effective before the burnout is entrenched.
Cognitive Warning Signs
The cognitive early warning signs of NCLEX burnout are changes in study session quality rather than changes in study session duration. The candidate who is beginning to burn out notices that they are reading the same sentence repeatedly without processing it — not because the sentence is difficult but because working memory is not holding the words long enough for comprehension to occur. They find that clinical scenarios that would previously have produced an immediate clinical impression now require multiple reads and still do not yield clear reasoning direction. They notice that rationale explanations that make complete sense while reading them do not produce any durable encoding — the clinical principle is clear in the moment and inaccessible five minutes later. They find that their sessions of 50 practice questions are producing the same clinical reasoning errors in the final 20 questions that they had at the beginning of preparation — not because the content is unfamiliar but because cognitive fatigue is degrading the application of reasoning frameworks that are otherwise available. These cognitive signs are distinct from content knowledge gaps and respond to rest and recovery rather than to additional content study.
Emotional Warning Signs
The emotional early warning signs of NCLEX burnout are more subtle and more commonly misattributed than the cognitive ones. A candidate developing NCLEX burnout experiences a progressive reduction in the emotional variability that preparation normally produces — the small satisfactions of understanding a difficult concept, the discouragement of a poor practice session, the encouragement of tracking accuracy improvement, and the motivated engagement of a productive day all flatten toward a pervasive emotional neutrality. This emotional flattening — sometimes called anhedonia in clinical language — means that positive preparation experiences stop producing the motivational lift they previously did and negative experiences stop producing the corrective urgency they previously would. The candidate feels neither particularly good nor particularly bad about preparation; they feel nothing in particular, which makes beginning each session harder because the motivational fuel that previously came from emotional engagement with the process is no longer generating the ignition that starting requires. Increased irritability — disproportionate frustration with minor preparation setbacks, difficulty managing the normal emotional experience of difficult questions — is another early emotional signal, produced by the reduced prefrontal cortex regulatory capacity that chronic stress creates.
Behavioral Warning Signs
NCLEX burnout’s behavioral warning signs are the ones most likely to be identified as preparation discipline failures rather than as physiological recovery signals. The candidate who is burning out finds that session start times drift progressively later in the day despite genuine intentions to begin earlier — the activation energy required to begin a preparation session has increased because the nervous system’s motivational systems are depleted. Question session length decreases not from lack of time but from inability to sustain clinical reasoning quality beyond 20 to 30 minutes — the candidate abandons sessions early because continuing at degraded quality feels pointless. Sleep patterns change: either difficulty falling asleep due to ruminative thoughts about preparation adequacy and exam anxiety, or excessive sleep without restorative effect due to HPA axis dysregulation. Social withdrawal increases as the candidate reduces contact with friends and family to devote more time to preparation that is producing diminishing returns. These behavioral changes are not character deficits — they are the behavioral signatures of a physiological state that responds to specific recovery interventions, not to increased discipline.
Why the Instinctive Response to Burnout Makes It Worse
The instinctive response to NCLEX burnout — studying more, disciplining more, pushing through the fatigue — is the response that most consistently converts manageable early burnout into preparation-disabling advanced burnout. Understanding why the instinct is wrong redirects the response toward what actually works.
The More-Study Trap
When a candidate notices that their practice accuracy is declining and their study sessions are producing less clinical reasoning development than they did two weeks ago, the logical interpretation is that they need more preparation. This interpretation is wrong when the cause of the declining performance is cognitive depletion rather than preparation content gaps. More study hours in a cognitively depleted state produce more time spent studying without more clinical reasoning development. The cognitive capacities required for clinical reasoning development — working memory, complex problem-solving, information consolidation — are exactly the capacities that burnout impairs. A candidate who extends their daily study hours from six to eight in response to declining practice accuracy during NCLEX burnout is deepening the depletion that is causing the accuracy decline rather than addressing the content gaps they believe are responsible. This more-study trap is particularly common among high-commitment candidates who have never before experienced the diminishing returns of pushed-through cognitive fatigue because their preparation has not previously exceeded their recovery capacity.
The Guilt Cycle
NCLEX burnout frequently triggers a guilt cycle that compounds the original depletion with an additional psychological burden. The candidate who takes a rest day or reduces preparation intensity in response to burnout symptoms experiences guilt about the reduced preparation — which activates the stress response, elevating cortisol and further impairing the recovery that rest was intended to provide. The cortisol elevation from guilt-driven anxiety about not studying enough actively impedes the hippocampal function and HPA axis restoration that adequate rest should produce. A candidate who spends a rest day ruminating about whether they are studying enough is not resting — they are sustaining the stress activation that caused the burnout while adding guilt as an additional stressor. Breaking the guilt cycle requires explicitly naming the rest period as a legitimate, medically-sound recovery intervention rather than as an indulgence that needs to be compensated for with additional preparation afterward. Rest is preparation. Recovery is preparation. The nervous system that emerges from a genuine rest period with restored cognitive capacity will produce more clinical reasoning development per hour of subsequent study than the depleted nervous system would have produced across twice as many hours without rest.
The Isolation Trap
NCLEX burnout candidates frequently respond to their depleted state by withdrawing from social connection to devote more time to preparation — a response that removes one of the most evidence-supported recovery mechanisms available. Social connection — not preparation conversation, but genuine non-nursing personal engagement with people the candidate cares about — is a direct neurobiological recovery mechanism. It reduces cortisol, activates the parasympathetic nervous system, and produces the oxytocin and serotonin release that directly counters the HPA dysregulation of burnout. A candidate who eliminates social contact to study more hours is removing a physiological recovery resource in exchange for additional depleted-quality study time — a trade that produces more depletion rather than more preparation. The most effective recovery from NCLEX burnout consistently includes intentional social reconnection as a component alongside reduced preparation intensity, sleep prioritization, and physical movement.
The NCLEX Burnout Recovery Protocol
Recovery from NCLEX burnout requires a specific multi-component protocol applied consistently rather than a single rest day followed by a return to the preparation intensity that produced the burnout. The protocol has three phases: acute recovery, preparation restructure, and sustainable reengagement.
Phase 1: Acute Recovery — Two to Three Days
The acute recovery phase of NCLEX burnout intervention requires complete temporary disengagement from NCLEX preparation activity — not reduced preparation, not passive content review, but complete disengagement. Two to three days without practice questions, without rationale review, without content study, and without preparation planning is the minimum acute recovery period for burnout that has moved beyond early warning signs. During the acute recovery phase, the priority activities are sleep (seven to nine hours per night, maintained without an alarm if possible), physical movement (30 to 45 minutes of moderate aerobic activity per day — this is the most rapidly effective cortisol regulation and HPA restoration activity available), nutritional normalizing (eating at regular times with adequate protein and complex carbohydrates regardless of appetite changes), and social reconnection (genuine non-nursing time with people the candidate cares about). These activities are not rewards for completing preparation — they are the specific physiological interventions that restore the cognitive capacity that clinical reasoning development requires.
Phase 2: Preparation Restructure — One Week
After the acute recovery phase, NCLEX burnout has typically subsided enough to allow a return to preparation — but a return to the same preparation intensity and structure that produced the burnout will reproduce it within one to two weeks. Phase two of the recovery protocol restructures the preparation approach before returning to normal intensity: identify which specific preparation behaviors produced the unsustainable demand. Common burnout-producing preparation behaviors include: daily preparation sessions without any scheduled days off (preparation seven days per week produces accumulating deficit without recovery margin), sessions that routinely extend beyond three hours (diminishing returns appear at approximately 90 minutes of intensive clinical reasoning work and become negative returns by three hours), elimination of all non-preparation activities to maximize study time (this removes the recovery mechanisms that prevent burnout accumulation), and the absence of a defined preparation end time that allows preparation demands to expand into sleep and relationship time. The restructured preparation plan explicitly includes two non-preparation days per week, session time limits of 90 minutes to two hours with breaks between sessions, and scheduled recovery activities that are treated as non-negotiable preparation infrastructure rather than optional personal indulgences.
Phase 3: Sustainable Reengagement — Return to Full Preparation
Phase three of the NCLEX burnout recovery protocol is the gradual return to full preparation intensity — not an immediate resumption of pre-burnout preparation volume but a progressive increase over one to two weeks that allows the recovery physiological state to be maintained as preparation demands increase. Begin with 30 to 45 questions per day in the first week of reengagement, increasing to 50 to 60 by the second week, returning to full preparation volume (50 to 75 daily questions with weekly simulation) by the third week if no burnout recurrence signs appear. Monitor for the early warning signs identified above at every stage of reengagement — cognitive difficulty, emotional flattening, behavioral drift — and treat their reappearance as a signal to reduce intensity rather than to push through. The candidate who successfully recovers from NCLEX burnout and returns to sustainable full preparation is typically more efficient than they were before burnout because the recovery period has provided perspective on which preparation behaviors are sustainable and which are counterproductive.
Preventing NCLEX Burnout: Sustainable Preparation Architecture
The most effective NCLEX burnout intervention is prevention — building a preparation architecture that sustains cognitive and emotional capacity across the full preparation period rather than maximizing short-term preparation intensity at the cost of long-term recovery capacity.
The Recovery Day as Preparation Infrastructure
The single most effective NCLEX burnout prevention practice is the scheduled recovery day — two designated non-preparation days per week that are treated as non-negotiable preparation infrastructure rather than as days when preparation did not happen. Recovery days are not a concession to laziness or insufficient commitment; they are the physiological mechanism that prevents accumulating cognitive deficit from producing the declining preparation quality that precedes NCLEX burnout. A candidate who prepares intensively for five days and recovers fully for two produces more total clinical reasoning development across a six-week preparation period than a candidate who prepares at lower intensity for seven days without adequate recovery margin — because the five-day candidate’s sessions occur with full cognitive capacity while the seven-day candidate’s sessions occur with progressively depleting capacity after day three of each week. The recovery day prescription is specific: use it for physical movement, social connection, sleep, and genuine engagement with activities that are personally meaningful outside of nursing — not for passive nursing content review that feels like rest but maintains the stress activation associated with preparation.
The Session Length Limit
NCLEX burnout prevention requires a defined session length limit applied as a non-negotiable boundary rather than as a guideline that can be exceeded when motivation is high. Clinical reasoning development is most efficient in the first 60 to 90 minutes of an intensive preparation session — working memory is fresh, cortisol is in the optimal performance zone, and clinical associations are forming at maximum efficiency. Between 90 minutes and two hours, efficiency declines. Beyond two hours, the quality of clinical reasoning diminishes to the point where continued question practice reinforces the same errors rather than correcting them. A candidate who ends a preparation session at 90 minutes despite still feeling motivated is not wasting preparation time — they are banking the cognitive recovery that will make the next session’s first 90 minutes fully productive rather than beginning from a depleted baseline. The total preparation value across two 90-minute sessions separated by a break and a full night’s sleep exceeds the value of a single three-hour session.
Physical Activity as Mandatory Preparation Infrastructure
Regular physical activity is the most evidence-supported non-preparation activity for NCLEX burnout prevention — not because physical fitness is intrinsically related to nursing examination performance but because the neurobiological effects of aerobic exercise directly counteract the mechanisms of burnout accumulation. Thirty minutes of moderate aerobic activity reduces cortisol, increases BDNF (brain-derived neurotrophic factor) which promotes hippocampal neurogenesis and memory consolidation, improves sleep quality, reduces anxiety reactivity, and produces the dopaminergic activation that restores motivational capacity. These are the specific neurobiological conditions that clinical reasoning development requires and that NCLEX burnout destroys. A preparation schedule that includes 30 minutes of physical activity on five of seven days is not sacrificing preparation time to exercise — it is investing in the neurobiological conditions that make the remaining preparation time more cognitively productive than the same hours without physical activity would be.
- Sleep as the highest-priority preparation variable: Seven to eight hours of sleep per night is not a recovery luxury — it is the physiological process during which memory consolidation occurs (hippocampal replay of the day’s clinical learning), cortisol regulation is restored, and prefrontal cortex regulatory capacity is recovered. A candidate who sacrifices sleep to extend preparation hours is trading the memory consolidation of the preceding day’s learning for additional preparation hours whose cognitive quality is impaired by the sleep deficit. No hour of study is worth more than the memory consolidation that adequate sleep produces.
- Preparation pleasure as a sustainability mechanism: A preparation approach that contains no enjoyable elements — in which every study session is experienced as obligation, every question session as anxiety-producing, and every content review as joyless — is structurally more prone to burnout than one that includes preparation activities the candidate genuinely engages with. Choosing a question bank platform whose interface the candidate finds satisfying to use, selecting video content review channels whose presentation style the candidate genuinely enjoys, and structuring the preparation week to include some content areas the candidate finds interesting alongside the ones that feel like obligation are not indulgences — they are sustainability mechanisms.
- The comparison detox: Social comparison — checking peers’ question counts, comparing accuracy percentages, monitoring whose preparation is more intensive — is a specific NCLEX burnout accelerant that can be eliminated by deliberate disengagement from nursing student social media and preparation discussion forums that generate comparison content. Every candidate’s preparation profile is different, every candidate’s burnout threshold is different, and no peer’s preparation pace is a reliable guide to the correct pace for any individual candidate.
When NCLEX Burnout Signals Something More
For most candidates, NCLEX burnout is a preparation management challenge that responds to the recovery and restructuring protocol described in this guide. For some candidates, burnout is accompanied by or overlapping with a mental health presentation that requires professional support rather than preparation restructuring alone.
Distinguishing Preparation Burnout from Clinical Depression or Anxiety
NCLEX burnout and clinical depression share several features — depleted energy, reduced motivation, emotional flattening, sleep disruption — but they differ in their cause, scope, and treatment response. Preparation burnout is contextually specific: it is produced by the specific demands of NCLEX preparation and its symptoms are largely confined to that context. A candidate experiencing preparation burnout who spends a day completely away from nursing activities typically notices meaningful relief and a temporary restoration of mood and energy. Clinical depression is contextually broader: it affects functioning across multiple life domains, is not primarily improved by removing the preparation stressor, and does not respond adequately to rest and recovery interventions alone. Similarly, NCLEX-specific anxiety — anxiety that is focused on the exam and its implications — is distinct from generalized anxiety disorder or panic disorder, which produce pervasive anxiety that extends beyond the examination context and requires clinical treatment. If a candidate finds that the recovery interventions described in this guide produce minimal improvement after one to two weeks, or if their psychological state is significantly impairing functioning outside of preparation contexts — relationships, daily activities, sleep even on rest days — seeking support from a mental health professional or student counseling service is appropriate and is a preparation decision, not a personal failure.
The Exam Date Decision During Burnout
NCLEX burnout raises a specific and difficult question about the exam date: should a candidate who is experiencing significant burnout proceed to a scheduled exam date or extend the preparation timeline? The answer depends on the burnout severity and the timeline. A candidate in early burnout who has three or more weeks before the scheduled exam and who implements the recovery protocol promptly will typically restore adequate cognitive functioning before the exam date. A candidate who is experiencing significant cognitive and emotional impairment from advanced burnout with two or fewer weeks remaining before the exam faces a more complex decision. Proceeding to the exam in a significantly burnout-impaired cognitive state risks a failed attempt whose consequences — 45-day wait, retesting fees, psychological impact — are more costly than a two-to-four week preparation extension. The proceed-or-extend decision should be made using the readiness benchmarks rather than timeline pressure: if the four readiness benchmarks are met despite the burnout experience, proceed; if they are not, the burnout recovery period can be used to address both the physiological recovery and the remaining preparation gaps simultaneously.
Seeking Support Is a Preparation Decision
The most important message for any nursing candidate experiencing NCLEX burnout is that seeking support — whether from a mental health professional, a student counseling service, a trusted mentor, or a peer who has navigated the same experience — is a preparation decision and a professional strength, not a personal weakness. The clinical judgment that makes a skilled nurse is partly the ability to recognize when a situation requires resources beyond what is currently available and to access those resources appropriately. Applying that clinical judgment to one’s own preparation experience is a demonstration of the same professional competency the NCLEX is designed to measure. You do not have to be well to ask for help. You do not have to have exhausted all self-help options before reaching out. And the burnout you are experiencing does not predict the nurse you are becoming — it reflects the demands of a rigorous preparation process that many nurses before you have navigated and emerged from to pass the examination and build meaningful clinical careers.
Conclusion
NCLEX burnout is a physiological state — not a character failure, not insufficient commitment, and not evidence that nursing is the wrong career. It is the predictable result of sustained cognitive and emotional demand exceeding recovery capacity, and it responds to specific recovery interventions the same way any other physiological state does: with appropriate, timely, targeted treatment. The early warning signs — cognitive impairment during study sessions, emotional flattening, behavioral drift toward avoidance — are signals to act rather than push through. The instinctive push-through response deepens the depletion rather than resolving it. The three-phase recovery protocol — acute disengagement, preparation restructure, and gradual reengagement — restores the cognitive capacity that sustainable preparation requires. The prevention architecture — recovery days, session length limits, physical activity, and adequate sleep — builds the structural conditions that prevent burnout accumulation rather than managing it after it develops.
If you are reading this guide because you recognize yourself in the description of NCLEX burnout, the most important message is this: rest is not the opposite of preparation. It is the physiological mechanism that makes preparation possible. The nursing candidates who pass the NCLEX are not the ones who studied the most hours — they are the ones who studied with adequate cognitive capacity, maintained their recovery mechanisms, and arrived at the exam with a nervous system capable of the clinical reasoning the exam demands. Take the recovery seriously. Restructure the approach honestly. And know that the path through burnout to exam readiness is a path that many nurses before you have walked and completed.