NCLEX scoring is one of the most misunderstood aspects of the entire nursing licensing process — and the misunderstandings are not trivial. Candidates who believe that receiving more questions means they are failing, or that a difficult question streak signals poor performance, or that the exam ends when a specific percentage of questions has been answered correctly, are operating with a mental model of the test that does not match how NCLEX scoring actually works. These misconceptions generate unnecessary anxiety during the exam and lead to preparation decisions that do not optimize for what the scoring system actually measures.
The NCLEX uses a Computerized Adaptive Testing system built on Item Response Theory — a psychometric framework that estimates a candidate’s underlying ability level continuously throughout the exam rather than calculating a percentage of correct answers at the end. NCLEX scoring does not reward getting the most questions right. It rewards demonstrating, with statistical confidence, that your clinical competency level is above the passing standard. This distinction changes almost everything about how to interpret your exam experience and how to prepare effectively for the outcome the scoring system is designed to measure.
This guide explains NCLEX scoring from the ground up: how the CAT algorithm selects questions and estimates competency, what the passing standard is and how it is set, what the number of questions you receive actually indicates, how the Next Generation NCLEX formats affect scoring in 2026, how partial credit works for NGN items, and what your results report tells you if you do not pass. Understanding NCLEX scoring thoroughly before you sit the exam removes a significant source of in-exam anxiety and replaces it with a clear, accurate picture of what the system is measuring and how your performance is being evaluated.
How NCLEX Scoring Works: The CAT System Explained
The Computerized Adaptive Testing system that powers NCLEX scoring is built on a psychometric model called Item Response Theory. Understanding its core mechanics is the foundation for interpreting everything else about the exam — question count, difficulty patterns, and the final pass or fail determination.
What Item Response Theory Measures
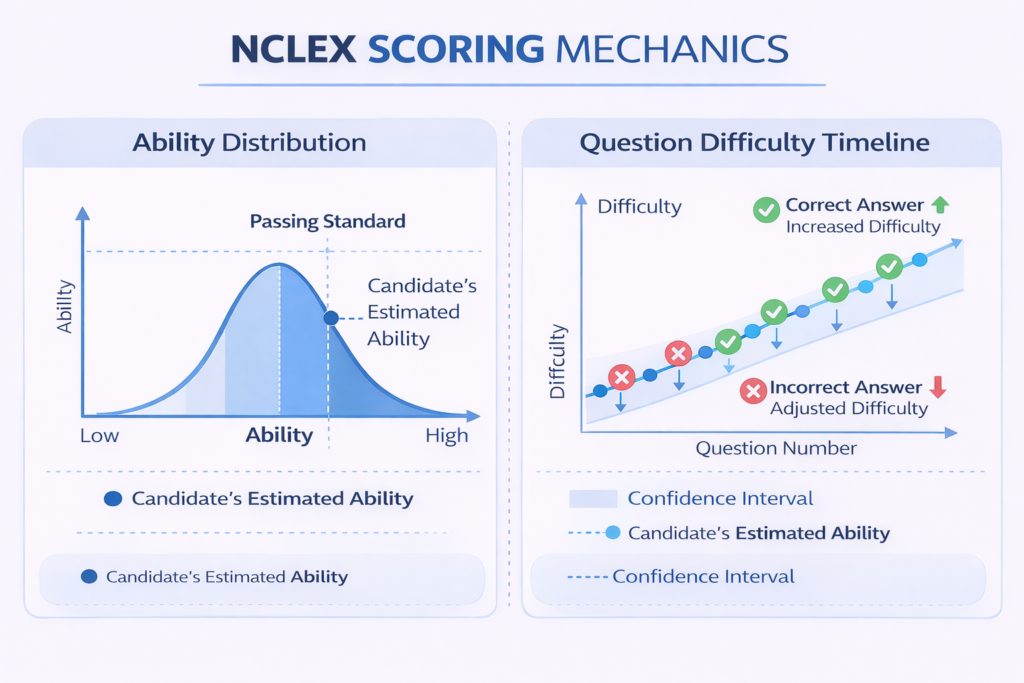
Item Response Theory is a statistical framework that models the relationship between a candidate’s underlying ability level and their probability of answering any given question correctly. Each question in the NCLEX item pool has three mathematically characterized properties: difficulty, discrimination, and guessing probability. Difficulty describes the ability level at which a candidate has a 50 percent chance of answering correctly. Discrimination describes how well the question distinguishes between candidates at different ability levels. Guessing probability accounts for the chance that a low-ability candidate selects the correct answer randomly. NCLEX scoring uses these properties to estimate your ability level from each response — not simply to count correct answers.
The critical implication for candidates is that NCLEX scoring is not a percentage calculation. There is no score of 72 percent or 88 percent. There is a continuous estimate of your ability level, expressed in logit units on a scale where the passing standard sits at a fixed point. Every response you give moves that estimate either upward or downward and narrows or widens the confidence interval around it. The exam ends when the confidence interval around your ability estimate is narrow enough that the system can determine with sufficient statistical certainty whether you are above or below the passing standard — not when you have answered a specific number of questions.
How the Algorithm Selects Questions
After each response, the NCLEX scoring algorithm updates its estimate of your ability level and selects the next question based on that updated estimate. The selection rule is maximum information: the algorithm chooses the question from the remaining item pool that provides the most statistical information about your ability at your current estimated level. In practice, this means the algorithm consistently targets questions near your estimated ability ceiling — questions you have approximately a 50 percent probability of answering correctly given your current estimate. This is why the NCLEX feels hard throughout the session for candidates performing at or above the passing standard. The difficulty is not constant — it is constantly adapting to where you are. Difficult questions are the algorithm’s response to strong performance, not a sign that something is going wrong.
The Confidence Interval and Exam Termination
NCLEX scoring terminates the exam when one of three conditions is met: the confidence interval around your ability estimate falls entirely above the passing standard, meaning the system is statistically confident you passed; the confidence interval falls entirely below the passing standard, meaning the system is statistically confident you did not pass; or the maximum item count of 150 questions is reached without a definitive determination having been made. In the third case, a final ability estimate is produced and compared to the passing standard to determine the result. The minimum item count of 75 questions exists because the algorithm requires a minimum number of responses to achieve any meaningful statistical confidence. Most candidates will receive between 75 and 135 questions — the distribution across this range does not directly indicate outcome direction.
The NCLEX Passing Standard: What It Is and How It Is Set

The passing standard is the fixed point on the NCLEX scoring scale that separates a passing result from a failing result. Understanding how it is set and what it represents clarifies what the exam is actually measuring — and why the passing standard reflects a clinical competency threshold rather than a competitive performance rank.
The Criterion-Referenced Standard
NCLEX scoring uses a criterion-referenced passing standard, not a norm-referenced one. A norm-referenced standard would set the passing cut score at a percentile rank relative to how other candidates perform — the top 70 percent pass, for example. A criterion-referenced standard sets the passing cut score at a fixed ability level determined by subject matter experts to represent the minimum clinical competency required for safe, effective entry-level nursing practice. This means the NCLEX passing rate is not fixed — it fluctuates based on the actual performance of each cohort of candidates relative to that fixed clinical standard. If a cohort of candidates is collectively better prepared, more will pass. If preparation is weaker across the cohort, fewer will pass. NCLEX scoring is not grading on a curve.
How the Passing Standard Is Determined
The NCSBN convenes panels of practicing nurses, nursing educators, and clinical experts at regular intervals to review and reset the passing standard through a structured psychometric process. Expert panelists independently rate each item in a sample set according to the probability that a minimally competent entry-level nurse would answer it correctly. These ratings are aggregated using the Angoff method or a similar criterion-setting approach to establish the ability level that represents minimum safe competency. The current passing standard for the NCLEX-RN was most recently evaluated and confirmed in the transition to the Next Generation NCLEX format. The standard reflects the consensus clinical judgment of practicing nursing professionals about what a new graduate nurse must be able to do safely — not an arbitrary difficulty threshold.
What Minimum Competency Actually Means
The phrase minimum competency is sometimes misread as meaning barely adequate. In NCLEX scoring terms it means something more specific: the ability level at which a nurse can be expected to practice safely without causing patient harm across the full range of entry-level nursing situations. This is a meaningful and demanding threshold. The exam is designed to confirm that candidates above the standard can be trusted to make safe clinical judgments — not to sort candidates by excellence, but to ensure that every licensed nurse who passes has demonstrated a foundational level of clinical reasoning that patient safety requires. Candidates who do not pass have not demonstrated that their clinical reasoning consistently meets this threshold — not that they are incompetent, but that their preparation has not yet brought their demonstrated competency above the standard the exam is built to verify.
What the Number of Questions You Receive Actually Means
No aspect of NCLEX scoring generates more candidate anxiety — and more misinformation in nursing student communities — than the question count. The correct interpretation is precise and important: the number of questions reflects the statistical efficiency of the exam for your particular response pattern, not a direct signal of pass or fail direction.
Why Some Candidates Receive 75 Questions
A candidate whose first 75 responses produce a confidence interval that falls entirely above or entirely below the passing standard receives exactly 75 questions. This happens when performance is consistent enough — consistently strong or consistently weak — that the algorithm achieves the required statistical certainty with the minimum item count. A candidate who receives 75 questions and passes demonstrated above-standard competency so clearly across those 75 items that additional questions would not change the determination. A candidate who receives 75 questions and does not pass demonstrated below-standard competency so consistently that additional questions would not change that determination either. The question count of 75 indicates statistical efficiency in NCLEX scoring — not a specific outcome direction.
Why Some Candidates Receive 150 Questions
A candidate who receives the maximum 150 questions did not produce a response pattern that allowed the algorithm to achieve a definitive confidence interval determination before the item limit. This occurs most often when a candidate’s performance hovers near the passing standard — answering some questions above the standard’s difficulty and others below it in a pattern that keeps the confidence interval straddling the threshold. It can also occur when early response patterns produce an ability estimate that is later revised significantly by subsequent responses, requiring the algorithm to collect additional data. Receiving 150 questions in NCLEX scoring is not evidence of poor performance — it is evidence that the exam required its full data-collection capacity to make a confident determination. Candidates who receive 150 questions and pass are not rare.
The Question Count Myth and Why It Persists
The myth that more questions means failing and fewer questions means passing persists because it contains a partial truth: candidates with very strong performance often receive fewer questions because consistent above-standard performance produces a narrow above-threshold confidence interval faster. But the logical error is in treating this correlation as a rule. NCLEX scoring is a statistical inference process, and candidates whose performance patterns are variable — performing strongly in some content areas and weakly in others — require more questions for the same statistical certainty. Variability in performance is not the same as below-standard performance, and the question count generated by variability is not the same as the question count generated by consistent below-standard performance. Do not attempt to predict your NCLEX scoring outcome from the question count alone.
NGN Formats and NCLEX Scoring in 2026: Partial Credit and Clinical Judgment
The Next Generation NCLEX formats introduced in 2023 changed the NCLEX scoring model in a meaningful way. Understanding how NGN items are scored is essential for every candidate preparing in 2026, because the partial credit mechanics of NGN scoring create both opportunities and risks that do not exist in traditional dichotomous scoring.
Dichotomous vs. Polytomous Scoring
Traditional NCLEX multiple-choice questions use dichotomous scoring: a response is either correct or incorrect, contributing a binary signal to the ability estimate. NGN formats use polytomous scoring for items where multiple correct selections are possible — extended multiple response questions, matrix questions, and enhanced hot spot highlighting. In polytomous NCLEX scoring, partial credit is awarded based on the number of correct selections made relative to the total correct options available. A candidate who selects four of five correct options in an extended multiple response item receives partial credit rather than a zero for the item. This partial credit signal contributes a more nuanced data point to the ability estimate than a binary correct or incorrect determination would.
Unfolding Case Studies and Sequential Scoring
Unfolding case study sets in the Next Generation NCLEX present six questions that follow a single patient scenario across a clinical encounter. NCLEX scoring for unfolding case studies evaluates each of the six questions independently — a candidate does not lose credit for all six questions by answering one incorrectly within the set. Each question maps to one of the six cognitive skills in the Clinical Judgment Measurement Model: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, and evaluate outcomes. The scoring contribution of each question reflects its item characteristics in the same Item Response Theory framework as traditional items. The unfolding structure means that a candidate’s performance across the six questions builds a composite picture of clinical judgment competency across the full CJMM sequence.
What NGN Scoring Means for Preparation
The polytomous scoring mechanics of NGN items have two direct implications for NCLEX scoring preparation. First, partial credit means that meaningful engagement with NGN items — carefully evaluating every option rather than guessing — is rewarded even when complete accuracy is not achieved. A candidate who thoughtfully selects four of five correct options contributes a stronger ability signal than a candidate who guesses and happens to select two correct options. Second, the CJMM-based structure of unfolding case studies means that clinical judgment competency across all six cognitive skill categories contributes to the ability estimate. Gaps in specific CJMM skills — particularly recognize cues and prioritize hypotheses, where many candidates underperform — affect NCLEX scoring in ways that are not visible from traditional question performance alone. NGN-specific preparation that develops all six CJMM skills is not optional in 2026.
Common NCLEX Scoring Misconceptions That Hurt Candidates
Misunderstanding NCLEX scoring mechanics leads to real preparation and in-exam behavior errors. The following misconceptions are the most widespread and the most consequential.
- Misconception — The NCLEX has a passing percentage: There is no passing percentage in NCLEX scoring. There is no score of 75 percent or 80 percent that constitutes a pass. The scoring system measures a continuous ability estimate and compares it to a fixed passing standard expressed in logit units. Candidates who ask ‘what percentage do I need to pass’ are asking a question the scoring system does not answer, because it is not how the system works.
- Misconception — Difficult questions mean you are doing well and easy questions mean you are failing: The adaptive nature of NCLEX scoring means question difficulty tracks your estimated ability level — not your performance direction relative to passing. A candidate performing near but below the passing standard will receive questions of moderate difficulty. A candidate performing well above the standard will receive very difficult questions. But a candidate performing near the passing standard who encounters a run of easier questions is not necessarily failing — the algorithm may be recalibrating after inconsistent responses. Question difficulty during the exam is not a reliable real-time performance indicator.
- Misconception — You can figure out your result by tracking right and wrong answers: Candidates sometimes attempt to count their correct and incorrect responses during the exam to estimate their NCLEX scoring trajectory. This is not possible for two reasons: the item scoring values vary based on item characteristics and polytomous partial credit mechanics, and the ability estimate is updated using a complex statistical function that cannot be approximated by simple tallying. The only meaningful signal available during the exam is to keep applying your best clinical reasoning to each question — not to count.
- Misconception — A run of wrong answers means you will fail: In NCLEX scoring, a sequence of incorrect responses does not produce a linear decline toward failure. The algorithm responds to incorrect answers by adjusting the ability estimate and selecting questions at a lower difficulty level — which gives the candidate the opportunity to demonstrate competency at a level where performance may be stronger. The adaptive recalibration process is specifically designed to find the level at which a candidate’s clinical reasoning is reliably accurate. A run of difficult questions answered incorrectly followed by easier questions answered correctly produces an ability estimate that reflects that pattern — not a simple failure determination.
- Misconception — The exam ends early because you passed: Some candidates interpret an exam that ends at 75 questions as confirmation of a passing result. This is false. NCLEX scoring terminates at 75 questions when statistical certainty is achieved — which can be certainty of either a passing or failing result. An exam ending at 75 is not good news or bad news in itself. It is information about the statistical efficiency of the session, not about the outcome direction.
Reading Your NCLEX Results: The Candidate Performance Report
If you do not pass the NCLEX, the most important document you will receive is the Candidate Performance Report. Understanding how to read it correctly is the difference between a repeat preparation that targets your actual gaps and one that repeats the same approach that did not produce a passing result the first time.
What the CPR Shows
The Candidate Performance Report does not show a numerical score. NCLEX scoring does not produce a numerical score for reporting purposes — it produces a pass or fail determination and, for candidates who do not pass, a performance profile relative to the passing standard across content categories. The CPR shows your performance in each of the eight major client needs categories from the NCSBN test plan: safe and effective care environment, management of care, safety and infection control, health promotion and maintenance, psychosocial integrity, basic care and comfort, pharmacological and parenteral therapies, reduction of risk potential, and physiological adaptation. For each category, your performance is indicated as near the passing standard, below the passing standard, or above the passing standard. The pattern across categories reveals where your clinical competency is below the threshold relative to the exam’s content weighting.
How to Use the CPR for Repeat Preparation
The most productive use of a Candidate Performance Report is as a precision targeting tool for a repeat preparation strategy. Categories marked below the passing standard represent content areas where your clinical knowledge and reasoning did not meet the minimum competency threshold. These areas require a different approach — not more questions from the same question bank, but genuine content re-study through a review book or tutoring resource, followed by targeted active recall practice, followed by clinical scenario practice questions specifically filtered to that content area. Categories marked near the passing standard represent areas where marginal improvement could meaningfully affect the overall ability estimate. Categories marked above the passing standard require maintenance but not intensive additional preparation. A repeat preparation structured around CPR data will outperform a repeat preparation structured around instinct or uniform volume increase every time.
The 45-Day and 90-Day Rule for Repeat Testing
Candidates who do not pass the NCLEX are subject to a waiting period before retesting. The standard waiting period is 45 days from the date of the failed exam before a new ATT is issued. Some jurisdictions impose a 90-day waiting period for candidates who have made multiple attempts. This waiting period is not wasted time — it is the preparation window for a structurally different approach based on CPR data. Candidates who use the full waiting period for targeted re-preparation consistently outperform candidates who rebook at the earliest available date without meaningfully changing their preparation strategy. NCLEX scoring rewards clinical competency above the passing standard — the retesting window exists to build it, not simply to accumulate more study hours doing the same things.
- Request your CPR immediately: The Candidate Performance Report is available through your state board of nursing or the NCSBN within a few weeks of a failed result. Request it as soon as it is available — do not wait until you have rescheduled your exam to begin analyzing your performance profile.
- Identify your deepest below-standard category: The content area with the lowest performance relative to the passing standard is the highest-priority target for re-preparation. Begin your repeat study schedule with intensive content review in this area before moving to secondary weak areas.
- Consider NCLEX tutoring for persistent gaps: If the same content categories appear below the passing standard across multiple attempts, the underlying issue is likely a clinical reasoning pattern rather than a content knowledge gap. NCLEX tutoring specifically designed to identify and correct clinical judgment errors produces faster improvement in these cases than additional self-directed content study.
- Do not ignore above-standard categories: Categories where your performance was above the passing standard still require maintenance during re-preparation. NCLEX scoring is holistic — consistent above-standard performance in strong areas contributes to the overall ability estimate and should not be allowed to decay during a preparation period focused heavily on weak areas.
Conclusion
NCLEX scoring is a psychometric system built to answer one precise question: does this candidate’s clinical competency meet the minimum threshold for safe, effective entry-level nursing practice? The CAT algorithm answers that question by continuously estimating your ability level, selecting questions that maximize statistical information about your position relative to the passing standard, and terminating the exam when sufficient certainty is achieved. It does not count correct answers, it does not grade on a curve, and it does not use the number of questions you receive to signal your outcome direction.
Understanding NCLEX scoring accurately changes how you experience the exam — difficult questions become evidence of strong performance rather than causes for alarm, an exam that ends at 75 questions is neither good news nor bad news until the result is confirmed, and a run of uncertain questions is a recalibration event rather than a failure signal. For candidates preparing for a first attempt, this understanding removes a significant source of in-exam anxiety. For candidates preparing for a repeat attempt, the Candidate Performance Report is the most valuable resource available — a precision map of where clinical competency fell below the standard and where to direct preparation to bring it above. In both cases, knowing how the system works puts you in a better position to perform within it.