NCLEX spaced repetition is the most evidence-supported memory consolidation method available to nursing candidates — and the one most rarely used correctly. The majority of candidates who use spaced repetition tools such as Anki use them in ways that produce a fraction of the method’s potential benefit: reviewing cards when it is convenient rather than when the algorithm schedules them, creating cards that test isolated facts rather than clinical reasoning, and treating the daily review session as a low-priority optional supplement rather than as a core preparation activity. The result is a spaced repetition system that accumulates cards without systematically closing the retrieval gaps it was designed to address.
Understanding why NCLEX spaced repetition works — at the level of memory consolidation science rather than as a vague recommendation to use flashcards — changes how the method is implemented in ways that significantly improve its effectiveness. The forgetting curve, the spacing effect, the testing effect, and the desirable difficulty principle are not abstractions — they are the specific mechanisms that make spaced repetition consistently superior to re-reading, highlighting, and summarizing for producing durable, exam-ready knowledge. When these mechanisms are understood, the preparation behaviors they require become not arbitrary discipline impositions but logical applications of how memory actually consolidates.
This guide provides the complete NCLEX spaced repetition framework: the memory science that explains why it works and why alternatives are less effective, the specific card design principles that make clinical reasoning retrievable rather than merely recognizable, the daily review protocol that maintains the method’s effectiveness across a full preparation period, the integration strategy that connects spaced repetition with question bank practice and rationale review, and the most common implementation mistakes that prevent candidates from extracting the method’s full preparation value.
The Memory Science Behind NCLEX Spaced Repetition
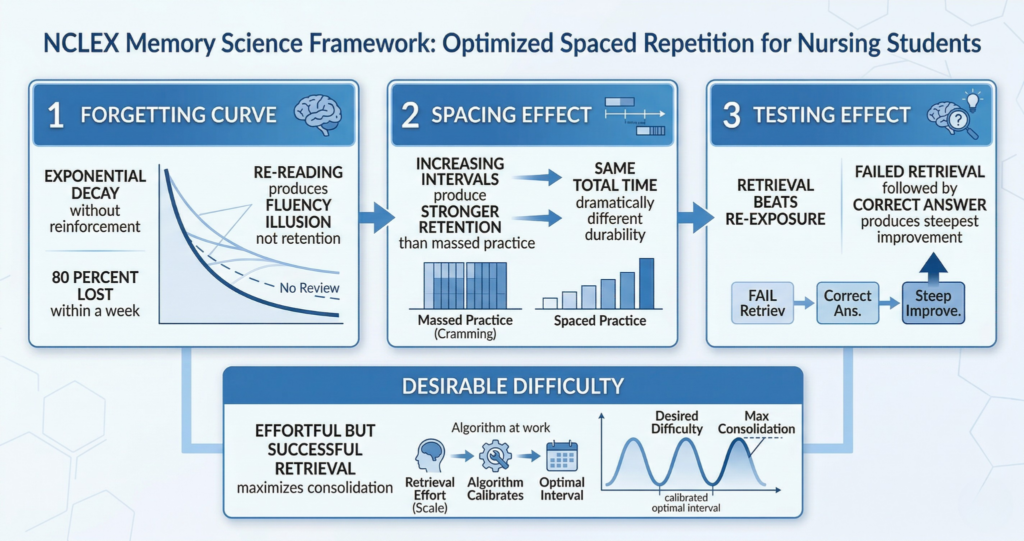
NCLEX spaced repetition is grounded in three converging memory science principles — the forgetting curve, the spacing effect, and the testing effect — that together explain why it produces durable knowledge more efficiently than any passive review method.
The Forgetting Curve and Why Re-Reading Fails
Hermann Ebbinghaus documented the forgetting curve in the 1880s: without any reinforcement, newly learned information decays exponentially from memory — approximately 50 percent is lost within an hour, 70 percent within 24 hours, and over 80 percent within a week of a single learning exposure. Every NCLEX candidate who has studied a clinical topic in depth on Monday and found it inaccessible by Thursday has experienced the forgetting curve directly. The instinctive response to forgetting is re-reading — returning to the source material and reading it again. Re-reading is the most common study method among nursing students and the least effective for producing durable memory. It produces the fluency illusion — material that has been read twice feels more familiar and better understood than material read once, creating a false sense of retention that collapses the moment retrieval is required under examination conditions. NCLEX spaced repetition addresses the forgetting curve not by re-exposing candidates to material but by scheduling retrieval practice at the specific intervals that produce maximum memory consolidation — exploiting the forgetting curve rather than fighting it.
The Spacing Effect: Why Intervals Matter
The spacing effect — one of the most robustly replicated findings in cognitive psychology — demonstrates that information reviewed at increasing time intervals is retained significantly longer than information reviewed in concentrated repeated sessions. Studying a clinical principle once on Monday, again on Wednesday, again on the following Monday, and again two weeks later produces substantially more durable memory than studying the same principle four times on Monday — even though the total study time is identical. The mechanism is that spaced retrieval requires the memory to be reconstructed from partial traces each time rather than simply refreshed from a currently active trace, which strengthens the neural encoding through the reconstruction effort rather than through passive re-exposure. NCLEX spaced repetition algorithms — implemented in tools like Anki — apply this principle precisely, scheduling each card for review at the interval that maximizes the consolidation benefit of the retrieval effort while minimizing the total time spent on review. A well-tuned spaced repetition system requires less total review time to produce more durable retention than any manually scheduled review system.
The Testing Effect: Retrieval Beats Re-Exposure
The testing effect — also called retrieval practice — demonstrates that attempting to retrieve information from memory produces stronger long-term retention than re-reading or re-studying the same information. The act of retrieval — even unsuccessful retrieval — strengthens the memory trace more than passive re-exposure to the material does. This is why NCLEX spaced repetition produces superior preparation outcomes to re-reading: every card review is a retrieval attempt rather than a re-exposure, and every retrieval attempt produces memory consolidation regardless of whether the retrieval succeeds or fails. Failed retrievals that are followed by correct answer review produce the steepest improvement in subsequent retrieval accuracy — which is why the cards most frequently answered incorrectly in a NCLEX spaced repetition system are the most valuable preparation assets rather than the most discouraging ones. They are the cards that are producing the most memory consolidation per review minute.
Desirable Difficulty: Why Easy Reviews Are Inefficient
The desirable difficulty principle completes the NCLEX spaced repetition science framework: memory consolidation is maximized when retrieval is effortful but ultimately successful. Reviews that are too easy — cards reviewed so frequently that they are always immediately accessible — produce minimal consolidation benefit because the retrieval requires no reconstruction effort. Reviews that are too hard — cards reviewed so infrequently that retrieval is almost always unsuccessful — produce frustration without the successful-retrieval consolidation that strengthens the trace. NCLEX spaced repetition algorithms are specifically calibrated to the desirable difficulty zone — scheduling each card at the interval where retrieval requires genuine effort but succeeds often enough to consolidate rather than frustrate. Candidates who override the algorithm by reviewing cards more frequently than scheduled (to feel more prepared) or less frequently than scheduled (because daily review feels tedious) are moving their reviews out of the desirable difficulty zone and reducing the method’s consolidation efficiency.
Designing NCLEX Spaced Repetition Cards That Build Clinical Reasoning

The most important determinant of NCLEX spaced repetition effectiveness after the review schedule itself is card design. Cards that test isolated clinical facts build recognition without clinical reasoning application. Cards designed to test clinical reasoning build the specific cognitive skill the exam measures.
The Clinical Scenario Prompt Format
Every NCLEX spaced repetition card should use a clinical scenario prompt on the front rather than a decontextualized fact question. The difference is the difference between these two card fronts: What are the signs of digoxin toxicity? versus A patient on digoxin reports nausea, vomiting, and seeing yellow halos around lights. Their potassium is 3.1 mEq/L. What is the priority concern, what assessment confirms it, and what is the first nursing action? The first format tests recognition of a list. The second format tests the clinical reasoning chain — identifying the presentation as digoxin toxicity, recognizing that hypokalemia potentiates toxicity and is the priority electrolyte concern, and applying the first nursing action of holding the digoxin and notifying the provider. The second card is harder to answer, takes longer to review, and produces more clinical reasoning development per review session. On exam day, the NCLEX will present the second format — a clinical scenario requiring application of clinical knowledge — not a list recognition question. NCLEX spaced repetition cards designed in the first format are preparing candidates for a different exam than the one they will sit.
The Back-of-Card Structure
The back of every NCLEX spaced repetition card should contain three components. First, the clinical principle: the specific clinical reasoning rule that makes the correct response correct — the mechanism that connects the presentation to the priority and the priority to the action. Digoxin toxicity is potentiated by hypokalemia because potassium and digoxin compete for the same Na-K-ATPase receptor site — low potassium increases digoxin binding and toxicity risk. Second, the correct response chain: the specific clinical action sequence in the correct priority order. Hold digoxin, obtain serum digoxin level and electrolytes, notify provider, anticipate Digibind order for severe toxicity. Third, the distractor analysis: the clinical reasoning error that would lead a candidate to select the wrong option. The most common distractor for digoxin toxicity is continuing the medication while monitoring, which is wrong because the toxicity threshold has already been exceeded and the drug must be withheld immediately. This three-component back structure makes every NCLEX spaced repetition card a complete clinical reasoning teaching unit rather than a simple fact-answer pair.
High-Yield Card Categories for NCLEX Preparation
The most valuable categories for NCLEX spaced repetition card creation are the clinical contexts that produce the highest density of exam questions and the highest frequency of clinical reasoning errors. Pharmacology scenario cards are the highest-yield category — each drug class generates scenario cards for priority adverse effects, monitoring parameters, patient education priorities, and contraindications. Prioritization scenario cards test the NCLEX’s most consistently tested reasoning skill — each clinical scenario with competing patient needs generates a card with the priority identification and the framework that produces it. Pathophysiology connection cards connect clinical presentations to the mechanisms that explain them — each body system finding generates a card connecting the finding to the underlying pathophysiology and the nursing action the mechanism requires. Safety assessment scenario cards cover the specific assessment findings that require immediate nursing action — each safety-relevant clinical change generates a card with the recognition criteria and the immediate response. NGN CJMM skill cards present clinical scenarios with the CJMM cognitive skill explicitly identified — each unfolding case study scenario generates cards for each of the six cognitive skills applied to that specific patient context.
The Daily NCLEX Spaced Repetition Review Protocol
The NCLEX spaced repetition system only delivers its full benefit when the daily review protocol is followed consistently — not when reviews are convenient or when the card count feels manageable, but every day without exception throughout the preparation period.
The Morning Review Window
The optimal placement of the daily NCLEX spaced repetition review session is first thing in the morning — before any other preparation activity and before any new content is encountered for the day. Morning review serves two functions simultaneously. First, it completes the due reviews before the day’s cognitive load accumulates — the retrieval effort required for due cards is cleanest in the morning cognitive state before the competing demands of clinical content study, question bank sessions, and life obligations reduce available working memory. Second, it reactivates the clinical reasoning network before the day’s primary preparation session, which makes the subsequent question bank practice more productive because the relevant clinical associations are already active rather than needing to be retrieved from cold. The morning review session should take 15 to 20 minutes for a mature deck in the middle of the preparation period — if it is consistently taking longer, the deck has accumulated more cards than the review schedule can sustain and card creation should be temporarily paused until the review backlog clears.
The Card Creation Session
NCLEX spaced repetition cards are created in a separate session from the daily review — typically at the end of the primary preparation session after question bank practice and rationale review are complete. The card creation trigger is the four-question rationale protocol’s transfer question: any clinical principle extracted from a rationale that was not previously consolidated — any principle that the rationale taught rather than confirmed — becomes a card before the session ends. The target is five to eight new cards per primary practice session — enough to build the deck systematically without creating an unsustainable review backlog. At five cards per session, five sessions per week, across six weeks of preparation, 150 cards are created — a comprehensive personalized clinical reasoning library sourced entirely from the candidate’s own documented knowledge gaps. Each card represents a principle that was wrong, unclear, or surprising during a practice session, making the deck a precise map of the preparation gaps that spaced repetition closes.
Managing the Review Backlog
The most common implementation failure in NCLEX spaced repetition is the review backlog — the accumulation of overdue review cards that builds when daily reviews are skipped and eventually becomes overwhelming enough to cause the candidate to abandon the system entirely. The review backlog prevention rules are: complete the due review session before creating any new cards (reviews take priority over card creation), never add more than ten new cards in a single day regardless of how much new content was studied (daily new card limits prevent unsustainable growth in review volume), and resume the review session after any missed day immediately rather than skipping the overdue cards. A single missed day adds the previous day’s due cards to the current day’s review — typically 20 to 30 additional cards — which is manageable. Three missed days in a row add 60 to 90 overdue cards to the current day’s review — which feels overwhelming and triggers abandonment. The never-miss-two-in-a-row rule applied to NCLEX spaced repetition reviews prevents the backlog spiral that ends most review systems.
Integrating NCLEX Spaced Repetition With Question Bank Practice
NCLEX spaced repetition reaches its maximum preparation value when it is integrated with question bank practice as a two-phase clinical reasoning consolidation system — not when it is used as a standalone memory tool alongside question bank sessions that run in parallel without connection between them.
The Question-to-Card Pipeline
The question-to-card pipeline is the integration mechanism that connects question bank practice and NCLEX spaced repetition into a unified preparation system. Every rationale review session generates potential card material: clinical principles that were absent from the knowledge base (knowledge gap cards), clinical reasoning errors that produced incorrect selections (reasoning error correction cards), and correct-answer principles reached through different reasoning than the rationale teaches (reasoning gap cards). The four-question rationale protocol’s transfer question — does this rationale change how I will reason about similar questions — identifies which principles meet the card creation threshold. Those that do are converted into clinical scenario prompt cards using the three-component back structure before the session ends. Those that do not — principles already consolidated, confirming existing reasoning — are noted as confirmed and the session moves forward. This pipeline ensures that every practice session contributes not only to the accuracy trend data that readiness benchmarks track but also to the spaced repetition deck that consolidates the principles those sessions teach.
Cards From Rationale Review vs. Cards From Content Review
NCLEX spaced repetition cards have two sources in a complete preparation system, and cards from each source have different characteristics that affect their review value. Cards from rationale review — created from practice question wrong-answer analysis — are scenario-grounded and clinical-reasoning-oriented because they originate from the clinical scenario format the exam uses. These cards produce the highest clinical reasoning development per review because they directly address the reasoning gaps that question performance has identified. Cards from content review — created from textbook, video, or review book study — are more likely to be fact-grounded if the card creation discipline is not carefully applied. The solution is applying the clinical scenario prompt format to content review-sourced cards with the same rigor as rationale-sourced cards: any content encountered in a review session that warrants a card becomes a scenario prompt, not a definition question. A content review session that produces only definition-format NCLEX spaced repetition cards is building a recognition-based review system rather than a reasoning-based one.
Measuring Spaced Repetition Progress
NCLEX spaced repetition progress is measured differently from question bank progress — not through accuracy percentages but through deck maturity indicators that reflect the health of the review system. Three maturity indicators matter. Average ease factor: Anki assigns each card an ease factor that reflects its difficulty — cards consistently answered correctly have high ease factors, cards frequently failed have low ease factors. A deck with an average ease factor below 2.0 across the card population indicates that too many cards are difficult, suggesting either insufficient daily review consistency or cards designed at a cognitive level too high for the current preparation stage. Daily review count: the number of due reviews per day should stabilize between 30 and 60 cards after three to four weeks of consistent card creation, with peaks during content-heavy weeks. If daily reviews consistently exceed 80 cards, new card creation should be paused and the backlog cleared. Retention rate: the percentage of cards answered correctly on their scheduled review day. A retention rate below 70 percent across the deck suggests the cards are being reviewed before they are sufficiently consolidated — often a sign that the algorithm settings have been customized incorrectly or that the daily review is not occurring at the scheduled time.
The Most Common NCLEX Spaced Repetition Mistakes
Even candidates who commit to NCLEX spaced repetition consistently make implementation mistakes that substantially reduce its preparation effectiveness. The following mistakes are the most common and the most costly in terms of preparation time invested without corresponding clinical reasoning development.
Using Pre-Made Decks Without Customization
Pre-made NCLEX spaced repetition decks — available through shared Anki deck repositories — provide a starting point that many candidates use without modification, treating the pre-made deck as a complete preparation system. The limitation of pre-made decks is significant: they are organized around generic clinical content rather than around the specific knowledge gaps and reasoning errors the individual candidate’s practice question sessions have identified. A pre-made deck covers digoxin toxicity because it is a high-yield NCLEX topic. A candidate-created card covers the specific distractor that the candidate selected when they missed the digoxin toxicity question and the specific reasoning error that distractor exploited. The candidate-created card is a precision gap-closing tool; the pre-made card is generic content coverage. Pre-made decks can supplement NCLEX spaced repetition by providing baseline coverage for content areas that have not yet been encountered in practice sessions, but they should never replace the candidate-created cards that directly address individual preparation gaps.
Reviewing Cards at the Wrong Time
NCLEX spaced repetition produces maximum consolidation benefit when cards are reviewed at the interval the algorithm schedules — not earlier and not later. Reviewing a card earlier than scheduled (because it feels important, because it was recently missed, or because the candidate wants to feel more prepared) moves the review out of the desirable difficulty zone toward the too-easy zone — the trace is still active from the recent exposure and the retrieval requires less effort, producing less consolidation. Reviewing a card later than scheduled (because a daily review was skipped) allows more forgetting to occur than the algorithm intended, pushing the review toward the too-hard zone where retrieval may fail entirely. The discipline of completing reviews when the algorithm schedules them — not when it is convenient or motivationally comfortable — is what preserves the method’s calibration. When life genuinely prevents a scheduled review, completing it as soon as possible after the scheduled time minimizes the deviation from the optimal interval.
Passive Card Review Without Active Retrieval
The most insidious NCLEX spaced repetition mistake is reviewing cards without genuine retrieval effort — reading the front of the card and immediately flipping to the back to confirm rather than generating the full clinical response from memory before revealing the answer. This passive review mode feels like studying because cards are being processed, but it produces almost none of the memory consolidation benefit that the testing effect requires. The retrieval attempt — however effortful, however uncertain — is what produces the consolidation. Flipping a card without attempting retrieval is equivalent to re-reading the back of the card from a new angle — it produces familiarity without durability. Before flipping any NCLEX spaced repetition card, generate the complete clinical response from the scenario prompt: the clinical principle, the priority nursing action, and the distractor type. If retrieval fails or is incomplete, flip and read the back fully. Mark the card as incorrect. The failed retrieval followed by full review is the highest-value interaction in the entire spaced repetition system.
- Mistake to avoid: Adding too many cards too quickly. A new card added is a new review obligation that compounds daily. More than ten new cards per day creates a review volume within two weeks that overwhelms the daily review capacity and causes system abandonment. Create five to eight new cards per session maximum and prioritize daily reviews over card creation volume.
- Mistake to avoid: Ignoring the algorithm’s ratings. After reviewing each card, the algorithm asks for an honest difficulty rating — again, hard, good, easy. Consistently rating cards as easy when they required genuine effort to retrieve, or consistently rating as good when the retrieval was actually uncertain, miscalibrates the scheduling intervals and degrades the system’s consolidation efficiency over time.
- Mistake to avoid: Stopping the system in the final two weeks before the exam. Some candidates suspend their NCLEX spaced repetition reviews in the final two weeks, believing that other preparation activities are more urgent. The final two weeks are when spaced repetition delivers its highest value — consolidating the clinical reasoning principles built across the preparation period into exam-ready retrieval strength. Continuing the daily review through the day before the exam is the correct approach; reducing daily question bank volume is the appropriate taper, not suspending the review system.
Building the NCLEX Spaced Repetition System from Week One
The full benefit of NCLEX spaced repetition accumulates over time — a system started in week one of a six-week preparation period produces substantially more consolidation by exam day than one started in week four. The following timeline builds the system progressively from the first day of preparation.
Week One: System Setup and Baseline Card Creation
In week one of NCLEX spaced repetition, complete the diagnostic assessment before any directed content study and create the first wave of cards from its rationale review. The diagnostic session of 75 to 100 questions with full rationale review will generate 30 to 50 card-worthy clinical principles — clinical facts that were absent, reasoning applications that failed, or prioritization distinctions that the rationale taught. Creating cards from this baseline diagnostic establishes the card deck around the candidate’s specific preparation gaps from the very first session, ensuring that the review system that builds across the preparation period is optimized for the individual rather than for the generic NCLEX candidate. Install Anki (free on desktop and Android, one-time purchase on iOS) and configure the daily new card limit to ten maximum and the daily review limit to 200. These settings prevent unsustainable growth while allowing sufficient daily exposure to new material.
Weeks Two Through Four: Building the Clinical Reasoning Library
From week two through week four, the NCLEX spaced repetition deck grows through consistent daily card creation from practice session rationale reviews and content study sessions. The morning review session expands from five to ten minutes in week one (small new deck) to 15 to 20 minutes by week three (maturing deck with significant review volume). By week four, a candidate creating five to eight cards per session across five sessions per week has added 100 to 160 cards to the deck — a substantial clinical reasoning library covering the specific gaps that four weeks of targeted practice sessions have identified. The daily review session at this stage is the most valuable 15 to 20 minutes of the preparation day because it is consolidating not generic nursing knowledge but the specific clinical principles that the candidate’s own documented reasoning gaps require.
Weeks Five Through Six: Consolidation and Final Calibration
In the final two weeks of preparation, NCLEX spaced repetition shifts from deck building to consolidation. New card creation slows as the practice sessions move from targeted content-filtered sessions to mixed-content and full simulation — generating fewer new card-worthy principles per session as the deck increasingly covers the knowledge base. The daily review session maintains its priority status and its 15 to 20 minute duration but now consists primarily of review cards reaching their longer-interval review due dates rather than newly created cards. These longer-interval reviews — cards from weeks one and two now scheduled for their 7-day or 14-day review — are the consolidation reviews that convert the clinical reasoning principles built during early preparation from recent memory into long-term memory. A candidate who has maintained consistent NCLEX spaced repetition across six weeks enters exam day with a clinical reasoning knowledge base that has been retrieved and consolidated multiple times at the optimal intervals — which is the maximum retrieval-ready memory state available for any preparation period of this length.
Conclusion
NCLEX spaced repetition is not a study tool — it is the application of memory consolidation science to clinical reasoning preparation. The forgetting curve explains why reviewing clinical content once is insufficient. The spacing effect explains why distributed review at increasing intervals produces more durable retention than massed review at equivalent total time. The testing effect explains why retrieval produces more consolidation than re-reading. The desirable difficulty principle explains why the algorithm’s scheduling is more effective than intuitive review decisions. Together these principles produce a preparation system that consolidates clinical knowledge and reasoning principles into exam-ready retrieval strength more efficiently than any passive review method.
The implementation that captures this value requires scenario-format card design rather than fact-format cards, daily review completion at the algorithm’s scheduled intervals rather than when convenient, the question-to-card pipeline that sources cards from documented preparation gaps rather than generic high-yield lists, and the consistency across the full preparation period that allows the compounding consolidation of the spacing effect to accumulate. Build the system from week one, maintain the daily review as a non-negotiable morning anchor, create cards from rationale review rather than from generic content lists, and let the algorithm manage the consolidation schedule. The result by exam day is a personalized clinical reasoning library that has been retrieved and reconsolidated multiple times at the optimal intervals — which is as close to exam-ready knowledge retention as memory science can produce.