NCLEX fundamentals of nursing is the content category that separates candidates who pass from those who plateau — not because it is the most complex material on the exam, but because it is the conceptual foundation that every higher-level clinical reasoning question is built on. A candidate who does not have a firm, retrievable grasp of the nursing process, safety principles, infection control standards, and basic patient care concepts will find that gaps in fundamentals quietly undermine performance in pharmacology, med-surg, and even NGN clinical judgment scenarios where these foundational concepts appear without being labeled as fundamentals.
The NCSBN test plan distributes fundamentals content across multiple client needs categories rather than grouping it in one discrete section. Safe and effective care environment, basic care and comfort, health promotion and maintenance, and safety and infection control all draw heavily on NCLEX fundamentals of nursing concepts. This distribution means that fundamentals is not a category you study once and move past — it is a layer of knowledge that runs underneath the entire exam and surfaces continuously in scenarios that appear to be testing other content areas. A cardiac nursing question that requires you to sequence your assessment correctly is testing fundamentals as much as it is testing cardiac pathophysiology.
This guide covers the essential NCLEX fundamentals of nursing concepts that appear most consistently across the exam: the nursing process as a clinical reasoning framework, Maslow’s hierarchy and its application to prioritization, safety and fall prevention, infection control and standard precautions, basic patient care and positioning, vital signs interpretation and abnormal findings, communication and therapeutic relationships, and documentation principles. For each area, the focus is on what the NCLEX actually tests — not on textbook comprehensiveness but on the clinical reasoning applications that scenario-based questions require.
The Nursing Process: The Clinical Reasoning Framework the NCLEX Tests in Every Question
The nursing process is the single most important concept in NCLEX fundamentals of nursing because it is the framework that underlies clinical reasoning in every question on the exam — not just questions explicitly about assessment or planning. Every NCLEX scenario that asks what the nurse does first, what the priority action is, or what should be assessed before proceeding is testing whether the candidate can apply the nursing process correctly to a clinical situation.
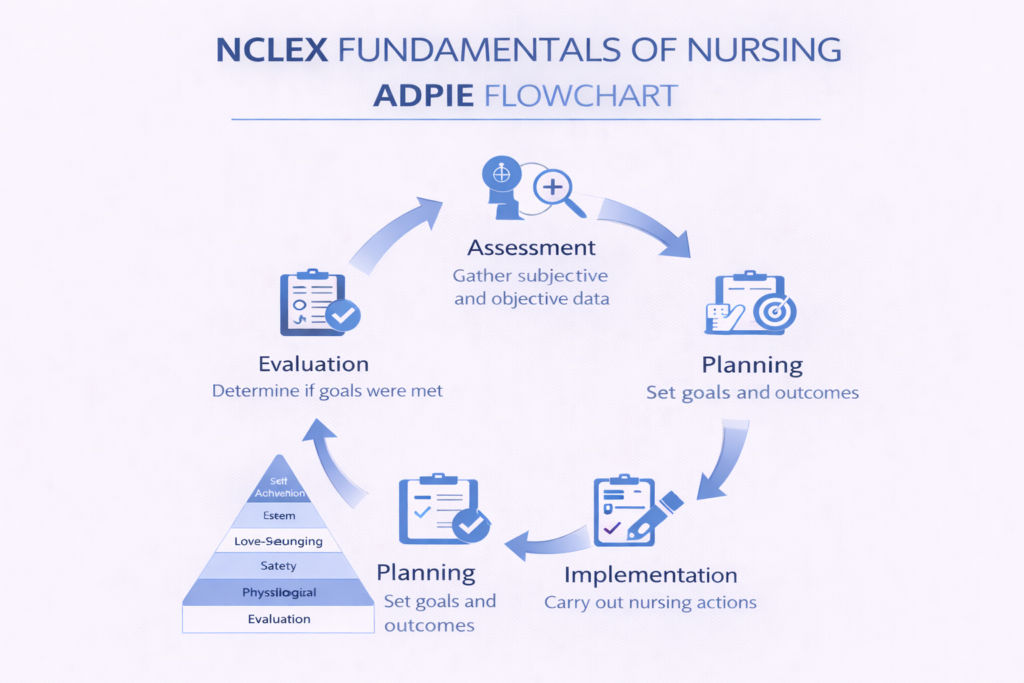
ADPIE: The Five-Step Framework
The nursing process follows five sequential steps: Assessment, Diagnosis, Planning, Implementation, and Evaluation. For NCLEX fundamentals of nursing questions, the most critical rule is that assessment always precedes intervention unless the patient is in immediate physiological danger. This rule eliminates a large proportion of incorrect answer options in clinical scenario questions — any option that involves implementing a nursing action before completing the relevant assessment is incorrect unless the scenario describes an active emergency requiring immediate action. When four answer options are presented and three involve implementation while one involves assessment, the assessment option is correct in the majority of non-emergency scenarios.
Assessment Comes First — With One Exception
The assessment-first principle in NCLEX fundamentals of nursing has a well-defined exception: when a patient’s airway, breathing, or circulation is in immediate jeopardy, the priority shifts from assessment to intervention. A patient who is not breathing requires airway intervention, not a full respiratory assessment. A patient in anaphylaxis requires epinephrine, not a detailed allergy history. Outside of immediate physiological emergencies involving the ABCs, the sequence of the nursing process is the correct sequence for clinical action — and questions that test this sequence appear throughout the exam in every content category.
Evaluation: The Most Commonly Neglected Step
Evaluation is the step of the nursing process most frequently underemphasized in NCLEX fundamentals of nursing preparation. NCLEX scenarios regularly test whether candidates can identify that an intervention was effective, identify that an intervention was not effective and requires modification, or identify the correct parameter to evaluate for a specific intervention. A candidate who knows that furosemide is a diuretic but cannot identify what assessment finding would indicate that the medication is achieving its intended therapeutic effect — decreased edema, increased urine output, decreased blood pressure — has incomplete functional knowledge of the intervention. Evaluation knowledge requires knowing not just what a nursing action is but what evidence of success or failure looks like after it is completed.
Maslow’s Hierarchy and Clinical Prioritization
Maslow’s hierarchy of needs is the second foundational framework in NCLEX fundamentals of nursing for clinical prioritization questions. When the nursing process has been applied and multiple patient needs have been identified, Maslow’s hierarchy determines which need takes priority. Physiological needs — airway, breathing, circulation, nutrition, elimination, pain — take priority over safety needs, which take priority over love and belonging needs, which take priority over esteem and self-actualization needs. For NCLEX purposes, this hierarchy translates directly into a triage and prioritization rule that eliminates incorrect answer options in every question where multiple patient needs compete.
Applying Maslow to NCLEX Prioritization Questions
NCLEX fundamentals of nursing prioritization questions typically present a patient with multiple concurrent needs — a physiological finding, an emotional or psychosocial concern, a safety issue, and a learning need. The correct answer addresses the most basic unmet need on the hierarchy. A patient who reports severe pain and also expresses anxiety about a pending procedure has both a physiological need (pain) and a psychosocial need (anxiety). Maslow directs the nurse to address pain first. A patient whose oxygen saturation is 88 percent and who also reports feeling lonely has both a physiological need (oxygenation) and a love and belonging need. Oxygenation is addressed first without question. The common error candidates make is selecting the psychosocial option because it appears more nursing-focused or empathetic — Maslow’s hierarchy is explicit that this sequence is incorrect.
When Physiological Needs Are Met: Safety Comes Next
NCLEX questions in which all physiological needs are already being addressed test the next tier of Maslow’s hierarchy: safety. Fall prevention, infection prevention, medication safety, and environment hazard identification are all safety-tier NCLEX fundamentals of nursing concepts. When a question presents a patient whose physiological status is stable and asks what the nurse addresses next, the correct answer is almost always the safety concern — ensuring the call light is within reach, raising bed rails for a confused patient, confirming a medication five rights check — rather than a psychosocial or educational intervention.
Safety and Fall Prevention: High-Yield NCLEX Fundamentals Concepts

Safety and fall prevention are among the most consistently tested NCLEX fundamentals of nursing concepts across all difficulty levels. They appear as primary question topics and as embedded clinical priorities within complex multi-system scenarios. The NCSBN test plan explicitly weights safety and infection control as a significant content category, and fall prevention is one of the most frequent topics within it.
Fall Risk Assessment and the NCLEX
NCLEX fundamentals of nursing questions on fall prevention most commonly test three competencies: identifying which patients are at highest fall risk, implementing the correct fall prevention interventions for a specific risk profile, and evaluating whether fall prevention measures are in place and effective. High-risk fall characteristics include age over 65, history of previous falls, altered level of consciousness or confusion, use of high-risk medications including opioids, benzodiazepines, antihypertensives, and diuretics, postural hypotension, impaired mobility or gait, and the immediate post-operative period. When a question asks which patient to assess first or which patient requires the most urgent fall prevention intervention, the patient with the highest concentration of these characteristics is correct.
Fall Prevention Interventions
The core fall prevention interventions tested in NCLEX fundamentals of nursing include keeping the bed in the lowest position with brakes locked, ensuring call light is within reach before leaving the room, orienting the patient to the environment and call light use at admission and after any room change, using non-slip footwear, clearing pathways between the bed and bathroom, using bed exit alarms for high-risk patients, ensuring adequate lighting especially at night, and scheduled toileting for patients with urgency or incontinence. NCLEX questions test whether the candidate selects the correct intervention for the specific clinical context — not whether they can list all possible interventions. A confused post-operative elderly patient who needs to void at night requires a combination of these interventions, and the question will test which the nurse implements first or which is most important.
Restraints: A Frequently Tested Safety Topic
Restraint use is a high-yield NCLEX fundamentals of nursing topic because it involves multiple competing priorities — patient safety, patient autonomy, and legal and regulatory requirements — that the exam tests through nuanced scenario questions. Key principles include: restraints are a last resort after all less restrictive alternatives have been tried and documented, a physician or licensed provider order is required before applying restraints, restraints must be tied to a part of the bed frame that moves with the bed rather than the side rail, neurovascular checks and skin assessment are performed every two hours for restrained extremities, and the order must be renewed every 24 hours. The most common NCLEX error on restraint questions is selecting restraint application before documenting that alternatives were attempted — which violates the last-resort principle.
Infection Control and Standard Precautions
Infection control is one of the highest-yield topic areas within NCLEX fundamentals of nursing, appearing consistently across all difficulty levels and in clinical scenarios from every nursing specialty. The NCSBN test plan explicitly lists safety and infection control as a weighted content category, and infection control questions test both knowledge of specific precaution types and clinical judgment about when and how to apply them.
Standard Precautions: The Foundation
Standard precautions apply to every patient encounter regardless of diagnosis, and this universality is itself a frequently tested NCLEX fundamentals of nursing concept. Standard precautions include hand hygiene before and after all patient contact, gloves for contact with blood, body fluids, non-intact skin, and mucous membranes, gowns when splashing or soiling of clothing is anticipated, masks and eye protection when splashing of body fluids to the face is possible, and safe needle handling and sharps disposal. The most important standard precaution concept for NCLEX is hand hygiene: it is the single most effective infection prevention measure, and it is required even when gloves are worn — gloves do not replace hand hygiene before donning or after removing them.
Transmission-Based Precautions: Contact, Droplet, and Airborne
Transmission-based precautions are added on top of standard precautions for patients with known or suspected infections transmitted by specific routes. Contact precautions — used for organisms like MRSA, VRE, C. difficile, and scabies — require gloves and gown for all room entry. Droplet precautions — used for influenza, pertussis, meningococcal disease, and mumps — require a surgical mask within three feet of the patient. Airborne precautions — used for tuberculosis, measles, varicella, and disseminated herpes zoster — require an N95 respirator, a negative pressure room with at least six to twelve air exchanges per hour, and keeping the patient’s door closed. NCLEX fundamentals of nursing questions on precautions most commonly test which precaution level is required for a specific organism or clinical presentation, and whether the candidate selects the correct PPE for that precaution type.
Donning and Doffing PPE: Sequence and Rationale
The correct sequence for donning and removing PPE is a consistently tested NCLEX fundamentals of nursing topic because errors in this sequence are a primary mechanism for self-contamination. Donning sequence: gown first, then mask or respirator, then eye protection, then gloves. Doffing sequence — designed to move from most contaminated to least contaminated: gloves first, then eye protection, then gown, then mask or respirator, with hand hygiene performed after glove removal and again after full doffing. The rationale for this sequence is that gloves are the most contaminated surface after patient care and must be removed first to prevent transferring contamination to less-contaminated PPE during subsequent removal steps.
Surgical Asepsis vs. Medical Asepsis
The distinction between surgical and medical asepsis is a foundational NCLEX fundamentals of nursing concept tested in clinical scenarios involving wound care, catheter insertion, IV line management, and sterile procedure performance. Medical asepsis — clean technique — reduces the number and spread of microorganisms but does not eliminate all of them. It applies to routine patient care, hand washing, and standard precaution measures. Surgical asepsis — sterile technique — eliminates all microorganisms including spores from objects and fields. It applies to any procedure that breaks the skin barrier or enters a sterile body cavity. NCLEX questions test whether candidates correctly identify which technique is required for a specific procedure and whether they recognize a break in sterile technique that requires stopping and re-establishing sterility before proceeding.
Vital Signs, Basic Assessment, and Patient Positioning
Vital signs interpretation and basic patient assessment are core NCLEX fundamentals of nursing topics that appear both as standalone questions and as embedded clinical data within complex scenarios. A candidate who cannot quickly recognize an abnormal vital sign pattern or identify its clinical significance will miss the priority cue in scenario questions where the vital sign data is the key to answering correctly.
Vital Signs: Normal Ranges and Abnormal Findings
Normal adult vital sign ranges for NCLEX fundamentals of nursing purposes: heart rate 60 to 100 beats per minute, respiratory rate 12 to 20 breaths per minute, blood pressure 90 to 120 systolic and 60 to 80 diastolic, temperature 36.1 to 37.2 degrees Celsius or 97 to 99 degrees Fahrenheit, and oxygen saturation 95 to 100 percent. For NCLEX clinical reasoning, the most important vital sign abnormalities to recognize and act on include: heart rate above 100 or below 60 with accompanying symptoms, respiratory rate above 20 or below 12, systolic blood pressure below 90 or above 180, temperature above 38.5 degrees Celsius indicating fever requiring assessment and intervention, and oxygen saturation below 95 percent requiring immediate position change and supplemental oxygen evaluation. The NCLEX tests not just recognition of abnormal values but the priority nursing response — which assessment follows, which intervention is initiated, and when to notify the provider.
Orthostatic Hypotension
Orthostatic hypotension is a high-yield NCLEX fundamentals of nursing concept tested in questions about falls, antihypertensive medications, dehydration, and post-operative care. It is defined as a drop in systolic blood pressure of 20 mmHg or more, or a drop in diastolic blood pressure of 10 mmHg or more, within three minutes of moving from a lying to a standing position. The nursing interventions for orthostatic hypotension include measuring blood pressure in lying, sitting, and standing positions before ambulation, instructing the patient to change positions slowly, dangling at the bedside before standing, and ensuring adequate hydration. NCLEX questions on orthostatic hypotension most commonly test whether the candidate identifies the correct sequence of measurement positions or the correct intervention before ambulating a high-risk patient.
Patient Positioning: Clinical Indications and NCLEX Rules
Patient positioning is among the most consistently tested NCLEX fundamentals of nursing topics because correct positioning is both a safety intervention and a therapeutic intervention depending on the clinical context. High-yield positioning rules include: semi-Fowler’s or Fowler’s position for patients with respiratory distress or difficulty breathing — elevating the head of bed 30 to 45 degrees optimizes diaphragmatic excursion and decreases the work of breathing. Left lateral Sims’ position for enema administration and rectal suppository insertion. Trendelenburg position — head down, feet elevated — is no longer recommended for hypotensive shock due to evidence of increased respiratory compromise and is not a current standard NCLEX answer for shock management. Elevating the head of bed 30 degrees for all patients receiving enteral tube feedings and maintaining this elevation for 30 to 60 minutes after a feeding reduces aspiration risk. For patients with increased intracranial pressure, the head of bed is elevated 30 degrees with the head in midline alignment to promote venous drainage.
Therapeutic Communication, Documentation, and Delegation
Therapeutic communication, accurate documentation, and safe delegation are three NCLEX fundamentals of nursing competency areas that appear throughout the exam and that many candidates underestimate because they seem less clinically complex than pathophysiology or pharmacology. These areas are not less important — they are directly tied to patient safety and are tested at application and analysis levels that require genuine understanding rather than simple recall.
Therapeutic Communication Principles
Therapeutic communication questions in NCLEX fundamentals of nursing test whether the candidate selects a response that facilitates the patient’s expression of thoughts and feelings rather than one that closes down communication, minimizes the patient’s concern, or shifts focus away from the patient. Techniques that facilitate therapeutic communication include open-ended questions, restating or reflecting the patient’s words to demonstrate active listening, acknowledging feelings without judgment, and using silence as an intentional communication tool. Techniques that block therapeutic communication — and that appear as incorrect answer options — include offering false reassurance such as ‘everything will be fine,’ giving unsolicited advice, changing the subject, using closed questions that require only yes or no answers, and expressing personal opinions about the patient’s choices or situation. A common NCLEX fundamentals of nursing question presents a patient expressing fear or grief and asks the nurse’s best response. The correct option acknowledges the feeling and invites the patient to continue — not to move toward problem-solving or reassurance prematurely.
Documentation Principles
Documentation questions in NCLEX fundamentals of nursing test accuracy, timing, objectivity, and the correct use of error correction procedures. Key rules include: document assessments and interventions promptly after they occur rather than in advance or at the end of a shift; use objective, measurable language rather than subjective interpretive language — ‘patient reports pain 7 out of 10 on numeric scale’ rather than ‘patient appears uncomfortable’; never document for another nurse or allow another nurse to document under your credentials; correct documentation errors by drawing a single line through the error, dating and initialing the correction, and writing the correct entry — never use correction fluid or obliterate the original entry; and if an event is not documented it is legally considered not done. Late entries require a specific notation as a late entry with the current date and time, the date and time of the original event, and the nurse’s signature.
Delegation: The Five Rights Framework
Delegation is a high-yield NCLEX fundamentals of nursing topic because it tests clinical judgment about scope of practice, patient acuity, and professional accountability simultaneously. The five rights of delegation provide the framework: right task — the task must be within the delegatee’s scope of practice and training; right circumstance — the patient’s condition must be stable enough that the task can be safely delegated; right person — the specific delegatee must have the demonstrated competency to perform the task; right direction and communication — clear, complete instructions must be given including expected outcomes and parameters for reporting back; right supervision and evaluation — the delegating nurse retains accountability and must follow up. NCLEX questions on delegation most commonly test which tasks can be safely delegated to a nursing assistant or LPN versus which must be performed by the RN. Assessment, care planning, evaluation of patient responses, and administration of IV push medications are RN-only responsibilities and cannot be delegated. Basic hygiene, vital sign measurement for stable patients, ambulation of stable patients, and specimen collection are appropriate nursing assistant tasks.
- Tasks an RN cannot delegate: Initial and ongoing assessment, nursing diagnosis, care plan development, evaluation of patient response to interventions, patient education requiring clinical judgment, IV push medication administration, and any task requiring professional nursing judgment about an unstable patient.
- Tasks appropriate for nursing assistants: Vital signs for stable patients, basic hygiene and grooming, feeding patients who do not have swallowing precautions, ambulation of stable patients, intake and output measurement, specimen collection, repositioning and comfort measures.
- Tasks appropriate for LPNs: Medication administration for stable patients by routes within their scope of practice, wound care for stable wounds, reinforcing patient education provided by the RN, monitoring of stable patients, and urinary catheter care.
Putting It Together: How NCLEX Fundamentals of Nursing Appears Across the Exam
NCLEX fundamentals of nursing content does not appear only in questions labeled as fundamentals. It surfaces as embedded clinical reasoning requirements in every specialty area. Understanding this cross-cutting presence is what allows a candidate to use fundamentals knowledge strategically throughout the entire exam rather than treating it as a discrete content section to study and move past.
Fundamentals Embedded in Med-Surg Questions
A cardiac nursing question that presents a post-operative patient with new-onset confusion, restlessness, and a heart rate of 108 is testing NCLEX fundamentals of nursing assessment skills as much as it is testing cardiac pathophysiology. The candidate must recognize that the assessment findings suggest a change in neurological and cardiovascular status, apply the nursing process to determine that a full assessment precedes any intervention, apply Maslow’s hierarchy to confirm that the physiological findings take priority over the patient’s expressed emotional distress about being in the hospital, and identify the correct priority nursing action — which is completing a focused assessment and notifying the provider, not administering a scheduled cardiac medication. The fundamentals framework is the scaffolding on which the med-surg clinical knowledge hangs.
Fundamentals Embedded in NGN Clinical Judgment Scenarios
Unfolding case studies and bow tie questions in the Next Generation NCLEX rely on NCLEX fundamentals of nursing competencies at the level of recognizing cues and prioritizing hypotheses — the first two cognitive skills in the Clinical Judgment Measurement Model. A candidate who cannot reliably identify which assessment findings are clinically significant, cannot apply the nursing process to determine the sequence of clinical action, and cannot apply Maslow’s hierarchy to prioritize among competing patient needs will struggle with NGN formats regardless of specialty content knowledge. The clinical judgment framework that NGN formats assess is built on the same foundational reasoning principles that NCLEX fundamentals of nursing develops.
A Targeted Fundamentals Review Approach
The most effective approach to NCLEX fundamentals of nursing review is not to re-read fundamentals textbook chapters but to use blank page recall and clinical scenario practice questions to confirm that these concepts are retrievable in applied form — not just recognizable when seen in a list. Test yourself: without notes, explain the five steps of the nursing process and the clinical decision rule that governs each transition between steps. Without notes, identify the correct precaution level, room type, and PPE for tuberculosis, MRSA, and influenza separately. Without notes, list the five rights of delegation and give one example of a task that is appropriate and one that is inappropriate for nursing assistant delegation. The retrieval difficulty you experience in these self-tests is the information that tells you where fundamentals review effort is most needed.
Conclusion
NCLEX fundamentals of nursing is not a section of the exam to check off and move past — it is the reasoning infrastructure that every other clinical question on the exam is built on. The nursing process determines the sequence of clinical action. Maslow’s hierarchy determines the order of priority when multiple patient needs compete. Standard and transmission-based precautions determine how safe care is delivered. Fall prevention and restraint principles determine how patient safety is maintained. Vital sign interpretation and positioning determine how assessment findings are translated into nursing action. Therapeutic communication, documentation, and delegation determine how safe, accountable, professional nursing practice is carried out.
A candidate who has a genuinely retrievable grasp of these NCLEX fundamentals of nursing concepts — one that is accessible under the cognitive load of a complex clinical scenario, not just recognizable when seen in a list — has built the clinical reasoning foundation that the exam measures at every difficulty level. Study these concepts actively, test your retrieval of them regularly, and apply them as the cross-cutting frameworks they are rather than as isolated topics. The fundamentals are fundamental for a reason — they are what safe nursing practice is built on, and they are what the NCLEX is designed to confirm you have mastered.