An NCLEX study group done well is one of the most powerful preparation accelerators available — and an NCLEX study group done poorly is a significant preparation liability. The difference between the two is not the quality of the candidates who participate but the structure and discipline governing how the group operates. An unstructured NCLEX study group quickly devolves into social time punctuated by occasional clinical discussion, consensus-based confidence-building that reinforces shared misconceptions, and the avoidance of difficult content areas because difficulty feels discouraging in a group context. A structured NCLEX study group with clear session formats, defined individual accountability, and an explicit rule against social comparison produces preparation benefits that self-directed study alone cannot replicate.
The preparation benefits of a well-structured NCLEX study group are specific and distinct from the benefits of individual preparation. Teaching a clinical concept to another person produces deeper encoding than studying it alone — the cognitive work of organizing knowledge into an explanation that makes sense to someone else forces the explainer to identify gaps in their own understanding that passive review conceals. Hearing a peer explain their clinical reasoning process for a question reveals approaches and frameworks the individual candidate had not considered. Discussing why all four options in a difficult question appear plausible — and working through the specific clinical reasoning that resolves the ambiguity — produces a more thorough analytical engagement with that question than individual rationale review typically generates. These are preparation benefits that require the group context to occur, and they are worth the coordination cost a structured NCLEX study group requires.
This guide provides the complete framework for building and running an effective NCLEX study group: the group composition principles that prevent the dynamics that destroy productivity, the session structure formats that extract maximum clinical reasoning development from group time, the individual accountability systems that prevent free-riding and ensure every member arrives prepared, the specific activities that leverage the group context most effectively, the warning signs of a group that has become counterproductive, and the decision framework for when individual preparation should take priority over group sessions.
Why Structure Makes or Breaks an NCLEX Study Group
The single most important determinant of whether an NCLEX study group produces preparation benefit or preparation cost is the presence or absence of explicit structure. Structure is not a formality imposed on a friendly group activity — it is the operational framework that prevents the three dynamics that destroy NCLEX study group effectiveness.
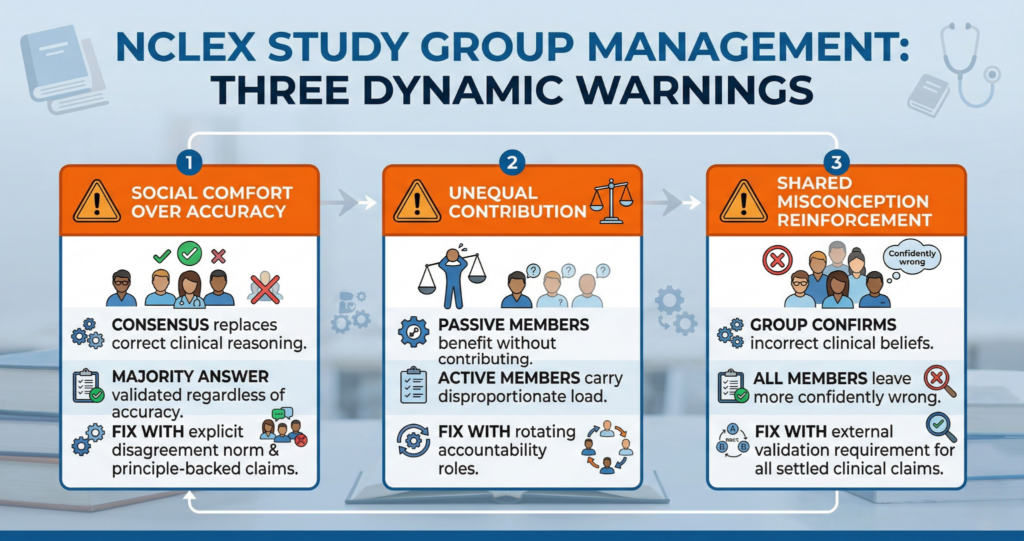
Dynamic 1: Social Comfort Over Clinical Accuracy
In any group of peers who share the stress of an upcoming high-stakes examination, there is a powerful social pressure toward mutual reassurance — the tendency to confirm each other’s answers, validate each other’s reasoning, and avoid disagreement that might make a member feel inadequate. An NCLEX study group without explicit norms for honest academic disagreement will gradually trend toward consensus rather than toward accuracy. When three group members select option C on a practice question and one selects option D, the social pressure in an unstructured group points toward validating the majority even when the minority option is correct. The correct answer is not democratic. The structure that prevents social comfort from overriding clinical accuracy is an explicit group norm: every clinical claim must be supported by a clinical principle, every answer selection must be accompanied by the reasoning that produced it, and disagreement is welcomed as the analytical engagement that produces the most thorough question discussion. An NCLEX study group that has established this norm produces better clinical reasoning from disagreement than an unstructured group produces from consensus.
Dynamic 2: Unequal Contribution and Free-Riding
An NCLEX study group without defined individual accountability roles produces a contribution gradient — some members carry disproportionate preparation load while others participate passively and benefit from the carrying members’ work without equivalent contribution. This dynamic is damaging both to the group’s preparation quality (passive participants extract information without developing their own clinical reasoning) and to group cohesion (carrying members eventually recognize the inequity and disengage). The structure that prevents unequal contribution is a rotating accountability role system: each session assigns specific preparation responsibilities to specific members before the session — topic preparation and explanation, question preparation and facilitation, rationale analysis responsibility, and session time management. Rotating these roles ensures that every member performs the high-cognitive-load preparation activities (preparing an explanation, selecting and facilitating practice questions) rather than only the passive reception activities.
Dynamic 3: Shared Misconception Reinforcement
The most clinically dangerous dynamic in an NCLEX study group is shared misconception reinforcement — when all or most group members share the same clinical misconception, group discussion confirms and deepens that misconception rather than correcting it. A group that collectively believes that antiparkinsonian medications are routinely prescribed alongside all antipsychotics — rather than specifically for EPS symptoms — will reinforce this belief through discussion and leave every member more confidently wrong than they were before. The structure that prevents shared misconception reinforcement is the external validation requirement: any clinical claim that the group accepts as settled truth during discussion must be verified against an authoritative external source — a rationale from the primary question bank platform, a review book page, or the NCSBN practice guidelines — before it becomes preparation content the group builds on. An NCLEX study group that validates claims against external sources rather than against group consensus is a preparation accelerator; one that uses group agreement as the validation standard is a misconception amplifier.
Group Composition: Size, Commitment, and Compatibility

An NCLEX study group’s effectiveness is partially determined before the first session by the composition decisions made during group formation. The following principles produce group compositions that sustain productive preparation across a full preparation period.
Optimal Group Size: Three to Five Members
The most effective NCLEX study group size is three to five members. Groups smaller than three lack the diversity of clinical reasoning perspectives and knowledge strengths that make group discussion more valuable than individual study — a two-person pair covers fewer clinical angles and has less redundancy when one member is poorly prepared for a session. Groups larger than five become logistically unwieldy, reduce individual air time during discussion, make scheduling significantly harder, and increase the likelihood that one or two members dominate while others participate minimally. Three to five members provides sufficient diversity of perspective for genuine clinical reasoning discussion, allows every member meaningful speaking time in a 90-minute session, and creates a scheduling flexibility that larger groups cannot maintain across a multi-week preparation period. If the available peer group is larger than five people with genuine commitment to structured preparation, consider forming two groups of three to four rather than one group of seven to eight.
Commitment Compatibility Over Friendship
The most common NCLEX study group formation mistake is selecting members based on friendship and social comfort rather than based on preparation commitment compatibility. A member who consistently arrives unprepared, misses sessions without notice, or treats the NCLEX study group as a social event rather than a structured preparation activity is a preparation liability regardless of how enjoyable their company is outside the group context. The preparation commitment screening conversation — discussing expected session frequency, individual preparation between sessions, acceptable absences, and group exit conditions — should occur before any member is invited into the group. Members whose expectations misalign significantly with the group’s standards for preparation discipline should not join the group, even when they are close personal friends. The preparation investment that each member makes in individual preparation between sessions determines what they contribute to group discussions; members who do not make this investment consume group time and energy without contributing clinical reasoning value.
Knowledge Strength Diversity
An NCLEX study group benefits from members whose clinical knowledge strengths are distributed across different content areas — a member with strong pharmacology and weak neurological content will contribute and receive different preparation value than a member with strong neurological content and weak pharmacology. This complementary knowledge distribution allows the group to leverage each member’s genuine content strengths in their role explanations while collectively covering the weaknesses that content diversity addresses. A group of members with identical knowledge strength profiles produces a narrower discussion range and a higher shared misconception risk than a group with diverse knowledge backgrounds. When forming an NCLEX study group, consider conducting individual diagnostic assessments before finalizing membership and evaluating whether the group’s collective content strength profile provides adequate coverage diversity.
The Session Structure That Maximizes Preparation Value
An NCLEX study group session without an explicit structure defaults to the lowest-cognitive-load activities — reviewing content the group already knows, discussing practice questions everyone answered correctly, and social conversation that consumes preparation time without producing clinical reasoning development. The following 90-minute session structure is specifically designed to allocate group time to the highest-cognitive-load preparation activities that group context enables.
The 90-Minute Session Template
The structured 90-minute NCLEX study group session has four sequential components. The first 10 minutes are individual accountability check-in: each member briefly reports the individual preparation completed since the last session — questions completed, accuracy in the targeted content area, and the top one or two clinical reasoning gaps identified from their week’s rationale review. This check-in creates individual accountability (members who did not prepare have to acknowledge it to the group), surfaces the content areas each member most needs from the group session, and establishes the group’s shared awareness of current preparation priorities before discussion begins. The following 25 minutes are the teach-back segment — the highest-value activity in any NCLEX study group session — in which the member assigned the topic role explains the assigned clinical content to the group from memory, without notes, while others listen, question, and correct inaccuracies against external reference. The central 40 minutes are collaborative question analysis: working through five to eight practice questions selected by the session’s question facilitator, with each question discussed using the four-question rationale protocol and every member explaining their reasoning before and after the answer is revealed. The final 15 minutes are session close: each member names one clinical principle learned during the session that changes how they will approach future questions, the next session’s topic and question preparation assignments are distributed, and any scheduling changes are confirmed.
The Teach-Back Segment: The Highest-Value Group Activity
The teach-back segment is the single most valuable component of any NCLEX study group session because it exploits the preparation benefit that only group context enables: the protégé effect. Teaching a clinical concept to another person requires the teacher to organize their knowledge into a logically sequenced explanation, anticipate the questions a listener might have, and identify the gaps in their own understanding when the explanation falters or when a group member’s question cannot be answered. This cognitive work produces deeper encoding of the clinical content than any passive review method and simultaneously reveals knowledge gaps that the teacher cannot identify through self-directed study alone. In the NCLEX study group teach-back segment, the assigned member explains the session topic from memory — the pathophysiology, the clinical presentation, the nursing priorities, and the priority action sequence — while other members listen attentively, ask clarifying questions, and provide gentle correction when clinical inaccuracies are identified. Every inaccuracy identified during teach-back is immediately verified against an external source before the corrected information is accepted. The combination of active explanation and honest peer correction produces clinical reasoning development that passive review and solo question bank work cannot replicate.
Collaborative Question Analysis Protocol
The collaborative question analysis segment of the NCLEX study group session uses a structured discussion protocol for each practice question that prevents the social comfort dynamic from producing premature consensus. For each question: every member answers independently in writing before any member reveals their selection. The session’s question facilitator then asks each member to reveal their answer and briefly state the one clinical reasoning principle that produced it — not yet discussing whether it is correct. With all answers and reasoning chains on the table, the facilitator reveals the correct answer and the group applies the four-question rationale protocol collaboratively: what clinical principle does the correct answer teach, why does each incorrect option fail for this specific patient, what reasoning error would lead a candidate to each wrong option, and does this question change how the group will approach similar scenarios? This structured discussion protocol ensures that members who answered incorrectly hear the reasoning of members who answered correctly before the rationale explanation, that every option’s failure mechanism is explicitly named, and that no member’s reasoning goes unexamined because social pressure discouraged it.
Individual Accountability Between Sessions
An NCLEX study group produces group preparation benefits only when every member arrives at each session having completed meaningful individual preparation between sessions. Group sessions cannot substitute for individual question bank practice, rationale review, and content study — they can only supplement and deepen the individual preparation that members bring. The individual accountability system defines what each member commits to completing between sessions and how that commitment is verified.
The Preparation Commitment Contract
At the formation of any NCLEX study group, every member should agree to and sign a written preparation commitment contract that specifies the minimum individual preparation expected between each group session. The contract covers: minimum weekly question bank sessions (at least three individual practice sessions of 50 questions each with full rationale review), content preparation for the assigned teach-back topic (sufficient depth to explain the content from memory without notes), preparation of any assigned questions for the collaborative analysis segment, and attendance standards (maximum one absence per four sessions with advance notice required). The written contract converts a verbal social agreement into a documented preparation standard that can be referenced when a member’s engagement falls below the group’s standard. A member who consistently fails to meet the contract terms should be given one direct conversation about the impact on the group before the group makes a membership change — but the conversation should occur rather than being avoided out of social discomfort.
The Pre-Session Accountability Report
The individual accountability check-in at the beginning of each NCLEX study group session is most effective when it uses a structured format that prevents social comfort from allowing members to represent their preparation as stronger than it was. Each member reports three data points: total practice questions completed since the last session, overall accuracy in the most recently targeted content area, and the single most important clinical reasoning principle identified from the week’s incorrect answer rationale reviews. These three data points are factual and verifiable — not impressionistic assessments of how well preparation is going. A member who completed 45 questions (short of the 150-question minimum), has 44 percent accuracy in renal nursing, and identifies hyperkalemia management as the key gap from the week’s incorrect answers has provided information that productively shapes the group’s discussion priorities for this session. A member who says I studied a lot this week has provided no actionable information and implicitly avoided accountability for a preparation shortfall.
The Partner Accountability System
Within the NCLEX study group, a paired partner accountability system creates a between-session check-in that maintains preparation momentum on days when group sessions do not occur. Each group member is paired with one other member for a two-week accountability partnership — pairs rotate every two weeks to prevent the accountability relationship from becoming too social and too comfortable to serve its function. Partners check in every other day between group sessions via a brief text message or message thread reporting: questions completed today, accuracy in targeted area, and one clinical principle from the day’s rationale review. The exchange takes two minutes per partner and produces four significant preparation benefits: it maintains daily question practice as a committed expectation rather than an optional activity, it ensures that preparation struggles are identified within 48 hours rather than discovered at the group session, it creates a low-stakes interpersonal accountability that is more motivating for many candidates than solo self-discipline, and it generates a continuous between-session awareness of each partner’s preparation status that enriches the quality of the accountability check-in at the next group session.
Warning Signs That a Study Group Has Become Counterproductive
Even a well-structured NCLEX study group can drift toward counterproductive dynamics across a multi-week preparation period. Recognizing the warning signs early allows corrective action before the group’s preparation value is permanently degraded.
Score Comparison and Performance Ranking
The first and most common warning sign that an NCLEX study group has become counterproductive is the emergence of score comparison culture — regular discussion of individual practice question scores, weekly accuracy trends, and relative performance between members. Score comparison in a study group produces two damages. For members performing above the group median, it generates complacency — if others are at 47 percent and I am at 58 percent, there is less felt urgency to close my own remaining gaps. For members performing below the group median, it generates anxiety and shame that reduces preparation quality and may cause them to disengage from the group rather than seek targeted help. Performance data in an NCLEX study group should be used for individual accountability (the pre-session report format described above) and for identifying shared weak areas that the group should address together — not for ranking members against each other. Any session in which score comparison is occurring should be redirected immediately to the structured protocol.
Preparation Drift Toward Comfort Content
A second warning sign is preparation drift — the group’s session topics and discussion questions gradually migrating toward content areas where most members feel relatively competent, because those sessions are more confident, more fluent, and more socially comfortable than sessions in genuinely weak areas. This drift is identifiable through the session topic log: if the NCLEX study group has spent three of the last four sessions on cardiovascular content that most members have above-standard accuracy in, while renal or pediatric content that the group’s diagnostics show as below standard has not been addressed in two weeks, the group is prioritizing comfort over preparation gap closure. The corrective action is returning to the data: the group’s collective diagnostic assessment should determine the session topic priority order, and the member assigned the topic role should have input into that priority order based on their personal gap profile, not their personal comfort with the topic.
Session Length and Frequency Creep
Session length creep — sessions that regularly extend significantly beyond the planned 90 minutes — and frequency creep — group meetings that occur so frequently that individual preparation time is displaced — are structural warning signs that the NCLEX study group’s organization has lost discipline. Extended sessions typically indicate that the structured session template is not being followed and social discussion is consuming preparation time. Excessive frequency — meeting four or five times per week — typically indicates that group sessions are being used as a substitute for individual question bank work rather than as a supplement to it. The most productive NCLEX study group meeting frequency is two sessions per week of 90 minutes each — sufficient for meaningful collaborative preparation benefit without displacing the individual practice that group sessions cannot replace. Any week in which more than three hours of preparation time is spent in group sessions is likely a week in which individual question bank practice has been displaced.
- Warning sign: Members arriving at sessions without having reviewed their individual performance data since the last session — indicating that the individual accountability between sessions is not occurring consistently. Address with a direct conversation about the contract terms before the next session.
- Warning sign: The teach-back segment being replaced with group review-book reading or watching a shared YouTube video — shifting the session from the highest-cognitive-load group activity to a passive reception activity that each member could have done individually. Restore the teach-back format explicitly.
- Warning sign: The collaborative question analysis segment consistently producing quick consensus without genuine disagreement — indicating either that the questions are too easy for the group’s current preparation level or that social comfort pressure is suppressing genuine analytical disagreement. Increase question difficulty and restate the disagreement norm at the beginning of the next session.
Conclusion
An NCLEX study group done well accelerates clinical reasoning development through the protégé effect of teach-back explanation, the analytical depth of structured collaborative question analysis, and the preparation accountability that defined individual commitment systems create. These benefits are only realized when the group has explicit structure — a session template that allocates time to high-cognitive-load activities, an individual accountability system that ensures every member arrives prepared, and group norms that prioritize clinical accuracy over social comfort. Without structure, the same group dynamics that make peer collaboration feel productive produce preparation costs rather than preparation benefits.
Form the group with three to five members selected for preparation commitment compatibility over friendship, using knowledge strength diversity as a secondary selection criterion. Run every session with the 90-minute template covering accountability check-in, teach-back, collaborative question analysis, and session close. Maintain individual accountability between sessions through the commitment contract, the structured pre-session report, and the partner check-in system. Monitor for the warning signs of drift toward comfort content, score comparison, and session length creep. The NCLEX study group that operates within this framework produces preparation benefits that self-directed study cannot replicate — and the nursing candidates who benefit most from group preparation are precisely those who are disciplined enough to insist on the structure that makes it work.