Smart NCLEX prep is not about studying more — it is about studying the right things in the right way at the right time. Most candidates who plateau during preparation are not plateauing because they are not working hard enough. They are plateauing because they are directing preparation effort toward the wrong targets. They study content areas where they already perform adequately because those sessions feel productive, avoid content areas where performance is low because those sessions feel discouraging, and generate high question volumes that maintain overall accuracy without closing the specific gaps the exam will expose. The result is weeks of intensive preparation that leaves the candidate at nearly the same readiness level they were at after week two.
The candidates who improve most rapidly during NCLEX prep are not the most disciplined or the most knowledgeable — they are the most precisely targeted. They know exactly which content areas are below the passing standard because they have measured it. They know exactly what type of clinical reasoning error is producing wrong answers in those areas because they have analyzed it. They know exactly what preparation activity closes that specific type of gap because they understand the difference between a knowledge gap and a reasoning gap and what each requires. And they execute a narrow, intensive, time-limited intervention on their highest-priority weak area before moving to the next one — rather than spreading preparation effort uniformly across everything and producing marginal improvement in everything.
This guide provides the complete smart NCLEX prep framework for turning weak areas into scoring strengths as efficiently as possible. It covers how to diagnose weak areas with precision rather than approximation, how to distinguish between the two types of performance gaps that require different interventions, the specific improvement protocols for each gap type, how to measure whether an intervention is working or needs to change, and how to integrate weak-area targeting into a complete preparation schedule that also maintains strong areas without allowing them to decay.
Step 1: Diagnose Weak Areas With Data, Not Intuition
The first step in smart NCLEX prep for weak area improvement is replacing intuition-based content prioritization with data-based content prioritization. Most candidates have an intuitive sense of which areas feel weakest — but the areas that feel weakest and the areas that the data shows are weakest are frequently not the same, and the data is always more reliable than the feeling.
Why Intuition Fails as a Diagnostic Tool
Intuitive weak-area identification in NCLEX prep is systematically biased in two directions. First, candidates tend to identify areas that feel unfamiliar as weak — content they did not study extensively in nursing school, topics they find conceptually difficult, or specialty areas they have not practiced clinically. But unfamiliarity on its own does not indicate poor performance on NCLEX practice questions, because some unfamiliar content is accessible through clinical reasoning frameworks even without specific content knowledge, and some familiar content produces systematic reasoning errors that accuracy metrics make visible only through data. Second, candidates tend to underestimate weakness in areas where they have studied extensively — the familiarity from repeated exposure creates a fluency illusion that masks retrievability gaps. A candidate who has reviewed pharmacology repeatedly may feel confident in it while producing below-standard accuracy on pharmacology scenario questions because the repeated review built recognition without building clinical application. Data from a diagnostic practice session reveals both of these biases simultaneously.
The Diagnostic Assessment Protocol
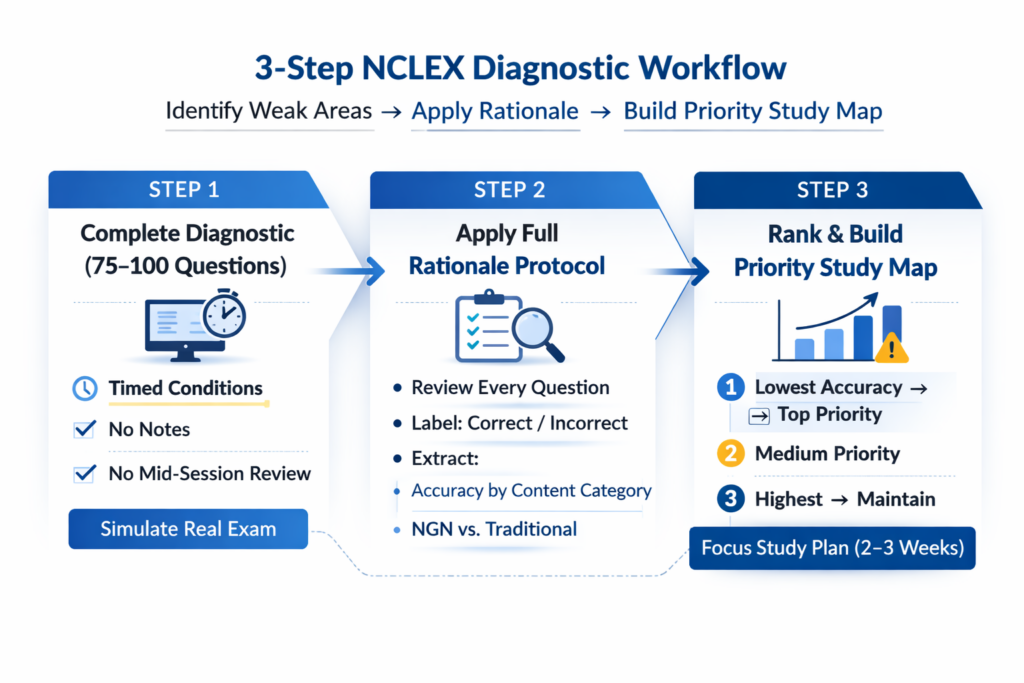
The most valuable single activity in smart NCLEX prep for weak area identification is a 75 to 100 question diagnostic assessment completed before any directed content study in a new preparation period or at the beginning of a targeted improvement phase. Complete it under timed, uninterrupted conditions without notes, references, or mid-session rationale review. Include a representative distribution of all major content categories and both traditional and NGN question formats. After the session, apply the full rationale review protocol to every question, then extract performance data organized by content category. Rank every content category by accuracy from lowest to highest. This ranking is your NCLEX prep priority map for the coming preparation phase — not what feels weakest, not what is most feared, but what the performance data shows is furthest below the passing standard.
NGN-Specific Diagnostic Data
A complete NCLEX prep diagnostic for weak area identification in 2026 must include format-specific accuracy separately tracked for NGN question types. Overall accuracy that masks significantly weaker NGN performance is one of the most common hidden preparation gaps — a candidate with 60 percent overall accuracy and 43 percent NGN accuracy has a specific format gap that the aggregate number obscures entirely. If the question bank platform separates NGN accuracy from traditional format accuracy in its analytics, review both metrics from the diagnostic session. If it does not, record NGN and traditional results separately in a performance log during the diagnostic session and calculate each category’s accuracy independently. A candidate whose diagnostic reveals both a below-standard content category and below-standard NGN accuracy needs to address both gaps — and the intervention for each is different.
Step 2: Identify the Type of Gap — Knowledge or Reasoning

Once weak areas are identified by data, smart NCLEX prep requires a second diagnostic step that most candidates skip: determining whether low accuracy in a given content area reflects a knowledge gap, a reasoning gap, or both. This distinction is the most important determination in the entire weak-area improvement process because the two gap types require fundamentally different interventions, and applying the wrong intervention to either produces minimal improvement regardless of effort invested.
What a Knowledge Gap Looks Like
A knowledge gap in NCLEX prep produces incorrect answers because the candidate did not have access to the specific clinical information the question required — the drug mechanism was not known, the clinical sign was not recognized as significant, the correct intervention sequence was not stored in retrievable form. Knowledge gap indicators include: incorrect answers accompanied by the experience of genuinely not knowing the content (not uncertainty about which option was correct, but genuine absence of the clinical principle the correct answer required); incorrect answers clustered around specific, identifiable clinical concepts within a content area rather than distributed across multiple concepts; and rationale review that reveals clinical facts the candidate had not encountered or studied. The correct NCLEX prep intervention for a knowledge gap is content review — not more practice questions on the same topic, but targeted study of the specific clinical content the rationale review reveals as missing, using a review book, video resource, or tutoring session. Questions alone cannot build knowledge that is not there; they can only reveal its absence.
What a Reasoning Gap Looks Like
A reasoning gap in NCLEX prep produces incorrect answers because the candidate had the relevant clinical knowledge but applied it incorrectly within the scenario — selected the right concept at the wrong nursing process step, prioritized the wrong patient need given the clinical context, applied the correct treatment to the wrong patient presentation, or did not recognize which clinical data in the stem was the priority cue. Reasoning gap indicators include: incorrect answers where the rationale review reveals that the candidate did know the underlying clinical content — they recognized the correct answer as clinically accurate after seeing it, but did not select it independently; incorrect answers that cluster around specific error types (process step errors, priority framework errors, patient context errors) rather than around specific content facts; and high-confidence wrong answers where the candidate was certain they were correct but selected a distractor. The correct NCLEX prep intervention for a reasoning gap is not more content review — it is targeted clinical reasoning practice with deliberate error pattern analysis, using the four-question rationale protocol and the reasoning error log to identify and correct the specific reasoning pattern driving incorrect selections.
The Mixed Gap: When Both Are Present
In practice, most significantly weak content areas in NCLEX prep contain elements of both gap types — some incorrect answers reflect missing knowledge and others reflect present knowledge applied incorrectly. The smart NCLEX prep approach to mixed gaps is sequential intervention: address the knowledge component first, then the reasoning component. Attempting to develop clinical reasoning application in a content area where foundational knowledge is still incomplete produces practice sessions where candidates cannot identify which aspect of their preparation is insufficient — which prevents the specific correction that either gap type requires. Complete one to two targeted content review sessions in the weak area before returning to practice questions, then resume practice questions with deliberate reasoning error analysis to address whatever reasoning gap persists after the knowledge foundation is established.
Step 3: The Knowledge Gap Intervention Protocol
When diagnostic data confirms that a content area is weak primarily because of missing or inaccessible clinical knowledge, smart NCLEX prep requires a specific knowledge-building intervention before returning to practice questions in that area. The following protocol produces the fastest knowledge gap closure available within a preparation timeline.
Active Content Review, Not Passive Re-Reading
The most common and least effective knowledge gap intervention in NCLEX prep is passive re-reading — opening a review book to the relevant chapter and reading through it sequentially. Passive re-reading produces recognition of familiar content without building retrievability under clinical reasoning conditions, which is precisely what NCLEX practice questions test. Active content review replaces passive reading with a cycle of read, close, and recall: read a defined content section — one body system component, one drug class, one clinical condition — then close all resources and generate from memory everything just studied. Write it, speak it, or think it explicitly — but generate it without resource access. Then open the resources and compare what was generated against what was missed. The gaps revealed by this blank-page recall are the specific clinical facts that need reinforcement — not a general impression that the topic needs more study, but precise identification of what the memory could not access under retrieval conditions. This targeted reinforcement is the most efficient knowledge gap intervention available in NCLEX prep.
The Condition-to-Intervention Recall Chain
For medical-surgical content gaps in NCLEX prep, the condition-to-intervention recall chain is the most clinically applicable active review format. After studying a specific condition — acute kidney injury, myocardial infarction, autonomic dysreflexia — generate from memory the complete clinical chain: the pathophysiology in two sentences of plain language, the priority assessment findings that present first and signal the highest urgency, the most dangerous complication and its early clinical signs, the first-line nursing intervention for each complication, and the relevant medications with their nursing assessment implications. This chain format mirrors the clinical reasoning structure that NCLEX scenario questions test — the ability to move from assessment findings through prioritization to intervention in a logically defensible sequence. A candidate who can generate this chain for a condition from memory has built the clinical reasoning architecture that NCLEX questions on that condition require. A candidate who can recognize the chain when it is presented to them in a question has not.
Spaced Reinforcement After Initial Review
Knowledge built through a single active review session decays rapidly without spaced reinforcement — the forgetting curve produces significant decay within 48 hours without a retrieval practice review event. Smart NCLEX prep for knowledge gap closure schedules spaced reinforcement automatically: review the content on the same day it is studied (end-of-session blank-page recall), review again 48 hours later, again at one week, and again at two weeks. Each reinforcement event should use the blank-page recall method rather than re-reading — the retrieval attempt itself is the reinforcement mechanism, not re-exposure to the source material. Converting key clinical principles from each study session into Anki cards with clinical scenario prompts automates this spaced reinforcement schedule — the Anki algorithm manages the retrieval timing, and the clinical scenario format of each card builds the application-level retrieval that NCLEX prep requires rather than isolated fact recall.
Step 4: The Reasoning Gap Intervention Protocol
When diagnostic data confirms that a content area is weak primarily because of clinical reasoning errors rather than missing knowledge, smart NCLEX prep requires a targeted reasoning correction intervention that is fundamentally different from content review. More content review for a reasoning gap produces no improvement — the knowledge is present, and the intervention needed is a change in how that knowledge is being applied under clinical scenario conditions.
Error Pattern Identification Before Question Practice
The first step of the reasoning gap intervention in NCLEX prep is identifying the specific error pattern driving incorrect answers before beginning additional question practice. Review the reasoning error log entries from the weak-area diagnostic session and categorize every incorrect answer by error type: process step error (implemented when assessment was correct, or assessed when evaluation was correct), priority framework error (selected psychosocial over physiological, or safety over ABC emergency), patient context error (applied correct knowledge to a different patient presentation), or knowledge gap (which redirects to the knowledge intervention protocol). The error type that appears most frequently is the specific reasoning correction target. A candidate whose incorrect pharmacology answers cluster around patient context errors — selecting the correct pharmacological action for the wrong patient presentation — needs targeted practice in reading clinical scenario data carefully and matching it to the correct patient context before engaging options. A candidate whose incorrect answers cluster around process step errors needs targeted practice in identifying action verbs and applying nursing process sequencing. The intervention is specific to the error pattern, not generic to the content area.
The Deliberate Error Correction Session
Once the dominant error pattern is identified, smart NCLEX prep for reasoning gap closure uses a deliberate error correction session: a 25 to 30 question practice session in the weak content area with the specific error type as the attentional focus. Before each question in the session, identify the element most relevant to the target error pattern — for process step errors, identify the action verb before reading options; for priority framework errors, identify all competing patient needs in the stem before reading options; for patient context errors, identify the specific clinical presentation characteristics that distinguish this patient from similar presentations before engaging options. After each question, apply the full four-question rationale protocol with particular attention to the error-type-specific analysis. The deliberate focus on a specific error dimension — rather than generic clinical reasoning improvement — produces faster reasoning pattern correction than unfocused practice because it gives the candidate a precise behavioral target rather than a general improvement goal.
The Accuracy Verification Check
After two to three targeted reasoning correction sessions in a weak NCLEX prep area, a verification check confirms whether the intervention is producing the intended improvement. Complete a fresh 25-question session in the same content area under standard practice conditions — no deliberate error-type focus, standard two-read and framework sequence approach. Compare accuracy to the pre-intervention baseline from the diagnostic. If accuracy has improved by five to ten percentage points and the dominant error type is appearing less frequently in the error log, the reasoning correction intervention is working and should continue for one to two more sessions before moving to the next weak area. If accuracy has not improved despite two to three targeted sessions, the reasoning gap explanation may be incomplete — the area may have a larger knowledge component than the initial diagnostic suggested, and a content review session should precede the next round of reasoning correction practice.
Step 5: Measure Progress and Adjust the Strategy
Smart NCLEX prep for weak area improvement requires systematic progress measurement — not the intuitive sense that things feel better but specific data confirming that accuracy in the targeted area is trending toward the passing standard. Progress measurement is what distinguishes a preparation strategy that is working from one that is producing effort without improvement, and it is what triggers the strategy adjustment that prevents weeks of continued ineffective preparation.
The Weekly Accuracy Trend Review
Every Sunday, review the past week’s practice question data from the NCLEX prep question bank platform and extract content area accuracy for each targeted weak area. Record this accuracy alongside the previous week’s number and identify whether the trend is upward, flat, or declining. An upward trend of three to five percentage points per week in a targeted weak area indicates that the intervention approach is working and should continue. A flat trend — accuracy in the same range for two consecutive weeks despite targeted practice — is a plateau signal that the current intervention approach needs to change: add a content review session if the plateau follows reasoning correction sessions, or switch to reasoning correction practice if the plateau follows content review sessions. A declining trend despite targeted practice signals something less common but more serious — performance may be declining due to fatigue, schedule compression, or an anxiety pattern that is interfering with practice quality rather than a preparation approach problem. Recognize declining trends within one week and investigate the cause before continuing the same intervention.
The Plateau Diagnosis Framework
A plateau in a targeted NCLEX prep weak area — accuracy that has not improved over two weeks despite consistent targeted practice — is one of the most important signals to respond to correctly rather than to push through with more of the same. Four plateau causes account for the majority of cases. First, the gap type was misidentified: the area was treated as a reasoning gap when it has a significant knowledge component, or vice versa. Solution: switch intervention type. Second, question volume is insufficient to reveal the improvement — 15 to 20 questions per week in a targeted area does not generate enough data for reliable trend measurement; increase to 25 to 50 targeted questions per week. Third, the rationale review is not being applied fully — improvement requires the four-question protocol applied to every question, and candidates who are completing questions without full rationale analysis are not receiving the clinical reasoning correction that produces improvement. Fourth, the area requires NCLEX tutoring to identify a reasoning pattern that self-directed analysis has not captured — some clinical reasoning error patterns are not visible in self-directed rationale review because they involve implicit assumptions or cognitive shortcuts that are not accessible to the candidate’s own introspection.
Moving On: When a Weak Area Has Improved Enough
Smart NCLEX prep weak area targeting requires knowing when to move on as clearly as knowing when to stay. The standard for moving from intensive targeted intervention to maintenance-level practice is: accuracy in the targeted area has reached 50 percent or above for two consecutive weeks of targeted practice, and the dominant reasoning error type has stopped appearing as the most frequent error type in the area’s log entries. At this threshold, reduce targeted session frequency from daily to every other day, and begin allocating preparation time toward the next highest-priority weak area from the diagnostic ranking. Continue weekly maintenance questions in the improved area — 15 to 20 questions per week — to prevent decay while the new target area receives intensive intervention. The maintenance questions serve two functions: they prevent the improved area from regressing under the forgetting curve, and they generate the analytics data needed to detect any regression trend early enough to address it before exam day.
Integrating Weak-Area Targeting Into a Complete NCLEX Prep Schedule
Weak-area targeting does not replace a complete NCLEX prep schedule — it provides the targeted intervention layer that sits within a broader preparation framework that also maintains strong areas, builds simulation stamina, and progresses toward readiness benchmarks on a defined timeline.
The 70-20-10 Daily Allocation
The most effective daily time allocation for smart NCLEX prep that balances weak-area targeting with broader preparation maintenance is the 70-20-10 split. Seventy percent of daily preparation time goes to the current highest-priority weak area: content review session or deliberate reasoning correction session in that area, followed by 25 to 30 targeted practice questions with full four-question rationale review. Twenty percent goes to maintenance practice in previously improved areas and mixed-content question sessions that build the clinical reasoning flexibility that content-filtered sessions alone cannot develop. Ten percent goes to NGN-specific format practice — ensuring that all five NGN question types receive consistent attention throughout the preparation period regardless of where targeted weak-area intervention is focused. This allocation keeps improvement momentum concentrated on the highest-priority gap while preventing strong areas from decaying and ensuring NGN competency builds continuously rather than being addressed as a last-minute addition.
The Weekly Simulation as a Progress Benchmark
Within a smart NCLEX prep weak-area targeting schedule, the weekly full simulation serves a specific progress measurement function beyond its stamina-building role. A 100-plus question mixed-content simulation completed on Saturday provides a weekly overall accuracy reading that reflects the cumulative effect of that week’s targeted weak-area improvement on the full performance profile. If the targeted area’s accuracy has improved during the week’s targeted sessions but the simulation’s overall accuracy has not improved or has declined, one of two things is occurring: the improvement in the targeted area is real but not yet reflected in a balanced mixed-content sample, or improvement in the targeted area is being offset by decay in a previously strong area that is not receiving maintenance practice. The simulation’s content area analytics breakdown — reviewed after full rationale review — reveals which situation applies and informs the following week’s 70-20-10 allocation adjustment.
The Three-Week Targeted Improvement Sprint
For candidates with three to four weeks remaining before the exam whose diagnostic reveals two or three specific below-standard content areas, smart NCLEX prep recommends a three-week targeted improvement sprint structured as follows. Week one: intensive intervention on the lowest-accuracy area — 70 percent of daily preparation time, full gap-type diagnosis and appropriate intervention protocol, daily targeted sessions. Week two: continue week one area at reduced intensity (40 percent) while beginning intervention on the second-lowest area (40 percent), with 20 percent maintenance mixed-content. Week three: consolidation — mixed-content simulation focus with targeted maintenance sessions in both improved areas and daily NGN format practice, weekly full simulations at exam-realistic length and timing. This sprint structure produces two targeted area improvements within three weeks while building the simulation stamina that the final preparation phase requires, and it generates the readiness benchmark data needed to confirm exam date appropriateness or trigger a timeline adjustment before booking fees are forfeited.
- Priority rule: Always target the lowest-accuracy content area first, regardless of how uncomfortable the content is or how much effort previous study has not improved it. The lowest-accuracy area produces the largest potential improvement in overall readiness per unit of preparation time — this is the most important allocation principle in all of smart NCLEX prep.
- Maintenance minimum: No content area that has previously tested above 55 percent should drop below 50 percent. A weekly monitoring scan that takes ten minutes reveals any area approaching this threshold in time to address it with two to three targeted maintenance sessions before the decay becomes significant.
- NGN non-negotiable: Regardless of how the weak-area targeting schedule is organized, at least 20 percent of daily practice questions should include NGN formats. NGN competency does not maintain itself through traditional format practice — it requires regular specific engagement with each NGN question type throughout the full preparation period.
Conclusion
Smart NCLEX prep for turning weak areas into scoring strengths is a five-step process grounded in data rather than intuition: diagnose with a timed diagnostic assessment and rank content areas by accuracy; identify whether each weak area reflects a knowledge gap, a reasoning gap, or both; apply the correct intervention protocol for each gap type — active content review with spaced reinforcement for knowledge gaps, deliberate error correction sessions for reasoning gaps; measure weekly accuracy trends and adjust the strategy when plateaus appear; and integrate weak-area targeting into a complete preparation schedule using the 70-20-10 daily allocation and weekly simulation as a progress benchmark.
The candidates who close the most ground in the least time during NCLEX prep are not the ones who study the hardest in their weak areas — they are the ones who study the right things in the right order with the right method for each specific type of gap. A knowledge gap that receives reasoning practice sessions does not improve. A reasoning gap that receives content review sessions does not improve. Both gaps, addressed with their appropriate interventions and measured weekly against objective accuracy data, can move from below-standard to above-standard within two to three focused weeks. That is the practical output of smart NCLEX prep: not more effort in the same direction, but precisely calibrated effort in the right direction for each specific gap you carry into preparation.